Back to 2024 Display Posters
Racial And Ethnic Disparities In Revascularization Options For Chronic Limb-threatening Ischemia
Caronae Howell, MD1, Wei Zhou, MD
1, Benjamin Brooke, MD, PhD
2.
1University of Arizona, Tucson, AZ, USA,
2University of Utah, Salt Lake City, UT, USA.
OBJECTIVES: Disparities in limb salvage outcomes amongst non-white patients with chronic limb-threatening ischemia (CLTI) are well established. Socio-economic disparities alone do not explain why clinical outcomes are inferior. This study was designed to compare anatomic patterns of disease and limb-salvage outcomes among patients from racial and ethnic groups undergoing first-time revascularization for lower extremity CLTI.
METHODS: We used the Vascular Quality Initiative registry (2012-2021) to identify patients who underwent peripheral vascular intervention (PVI) or infra-inguinal bypass (INFRA) for CLTI. Black, Hispanic/Latinx and American Indian/Alaskan Native (AINA) patients with CLTI were compared to White controls. Primary outcomes were incidence of 1-year major amputation, reintervention, and amputation free survival. Kaplan-Meier curves and Cox proportional-hazards models were used to assess the association between race and ethnicity and primary outcomes.
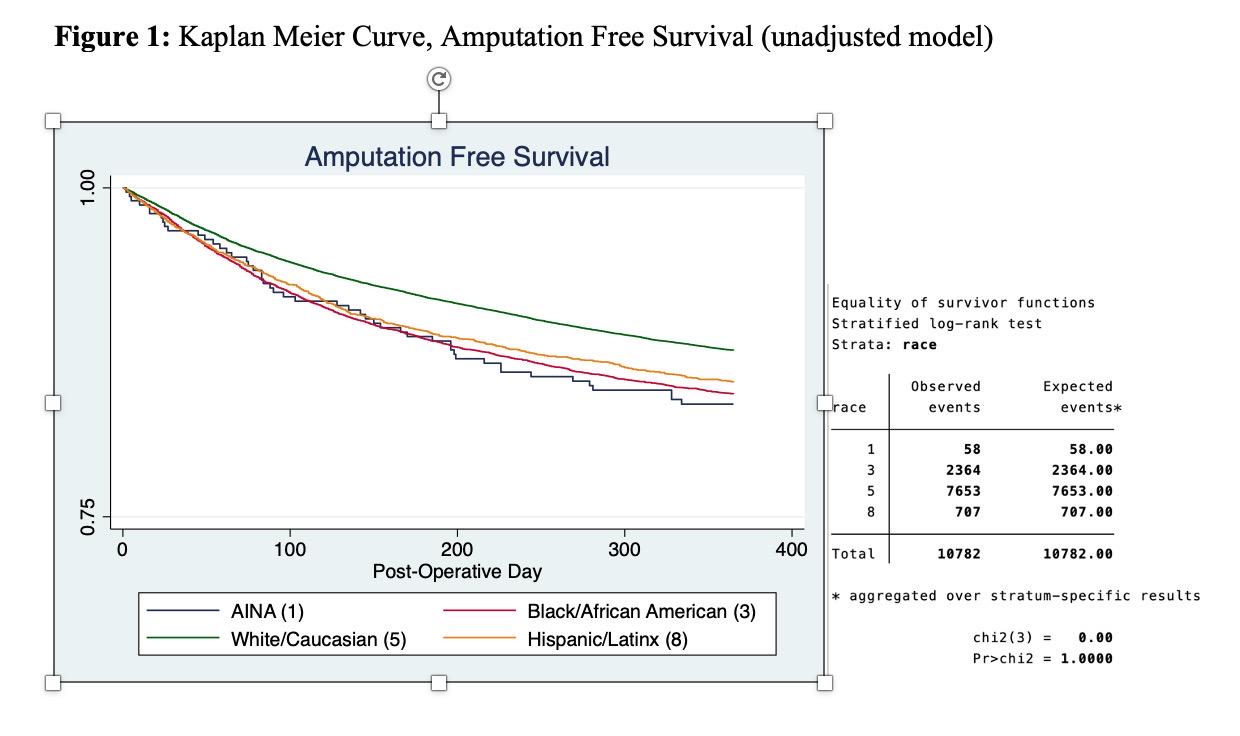
RESULTS: We identified 74,765 patients (70% PVI and 30% INFRA), composed of 72% White, 20% Black, 7% Latinx, and 1% AINA. Latinx and AINA patients were significantly more likely to present with tissue loss than White or Black patients (P<.001). Black, Latinx, and AINA patients had significantly increased rates of tibial/pedal intervention, technical failure, and number of arteries treated >1. On multivariate analysis of PVI, AINA patients were more likely to have tibial (OR 2.5, 95% CI 1.9-3.2) or pedal (OR 3.1, 95% CI 2.0-4.6) vessels treated. AINA and Black patients were more likely to have an unsatisfactory technical result. In the INFRA analysis, Black and Latinx patients fared worse in several areas, including tibial/pedal bypass target and use of non-vein graft. All minority groups experienced worse amputation-free survival and increased rates of major adverse limb events (Figure 1).
CONCLUSIONS: Non-white patients undergoing revascularization for CLTI were more likely to require tibial or pedal interventions. These findings suggest that disease severity at presentation, along with a requirement for more technically challenging interventions, may account for some of their disparities in limb salvage outcomes.

Back to 2024 Display Posters