Back to 2024 Display Posters
Transitions Of Frailty After Primary Dialysis Access Placement
Mark G. Davies, MD PhD MBA1, Joseph P. Hart, MD, MNL
2.
1Ascension Health, Waco, TX, USA,
2Medical College of Wisconsin, Milwaukee, WI, USA.
Objective: Establishing long-term hemodialysis access is an important component in long-term care for patients with End Stage Renal Disease (ESRD). The aim of this study was to analyze transitions in frailty-state among patients undergoing primary dialysis access placement.
Methods: Between 2018 and 2022, all patients undergoing a primary access placement were analyzed. Frailty was assessed by VQI-derived Risk Analysis Index (VQI-RAI). No pre-emptive access surgeries were included to allow for uniformity. Frailty was defined as a VQI-RAI score
> 35. Transition in frailty state between preoperative and follow-up measurement at 1 month, 6 months, and 1 year were analyzed. Patient characteristics leading to a transition in frailty state were analyzed using multivariable Cox regression analysis. Outcomes of maturation (successful progression to HD), re-intervention, functional dialysis (continuous HD for three consecutive months), and patency were examined.
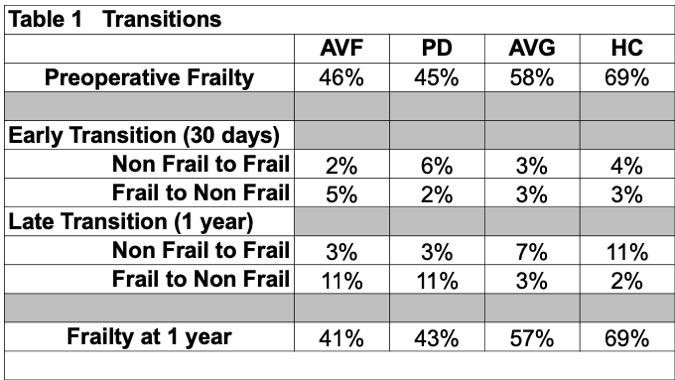
Results: 472 patients (56% female, mean age of 66�13yrs; mean�SD) underwent placement of arteriovenous fistula (AVF, 86%), peritoneal dialysis catheter (PD, 6%), arteriovenous graft (AVG, 4%) and long-term hemodialysis catheter (HC, 3%). 53% were considered frail on initial evaluation (Table 1). At 30 days, overall frailty decreased to 44%: 1% of patients moved from Non-Frail to Frail, and 2% of patients moved from Frail to Non-Frail. At 1 year, overall frailty increased to 43%: 2% of patients shifted from Non-Frail to Frail, and 5% of patients shifted from Frail to Non-Frail (Table 1). At one year, frailty increased by 5% in AVF, 2% in PD, and 1% in AVG and was unchanged in HC. Frailty at baseline, 30 days, and 1 year were associated with a high Charlson Comorbidity Index, poor maturation, and an increased number of procedures to achieve functional access. Shifting to a frail state postoperatively was associated with early thrombosis, decreased maturation, decreased survival, and lower functional dialysis at 1yr.
Conclusions: Dialysis patients have a high incidence of frailty prior to initiation of dialysis. Achieving non-catheter-based dialysis access stabilizes and improves frailty at one year compared to catheter-based dialysis. Shifting to a frail state is associated with poorer outcomes and should be considered when evaluating a patient for dialysis access

Back to 2024 Display Posters