Back to 2024 Display Posters
Evolution Of Approaches For CLTI Management After The Publication Of BEST-CLI
Celena M. Russell1, Sai Divya Yadavalli, MD
1, Gabriel Jabbour, MS
1, Lucas Souza-Mota, MD
1, Jorge L. Gomez-Mayorga, MD
1, Fahad Shuja, MBBS
2, Douglas W. Jones, MD, MS
3, Marc L. Schermerhorn, MD
1.
1Department of Surgery, Division of Vascular and Endovascular Surgery, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, USA,
2Division of Vascular and Endovascular Surgery, Mayo Clinic, Rochester, MN, USA,
3Division of Vascular and Endovascular Surgery, University of Massachusetts Medical Center, University of Massachusetts Medical School, Worcester, MA, USA.
OBJECTIVES:There are limited data available regarding how the findings of the BEST-CLI study have affected the treatment choice of surgeons dealing with Chronic limb-threatening ischemia (CLTI). Using the VQI database, this study evaluated changes in clinical practice that may have occurred after the publication of the BEST-CLI study outcomes in November 2022.
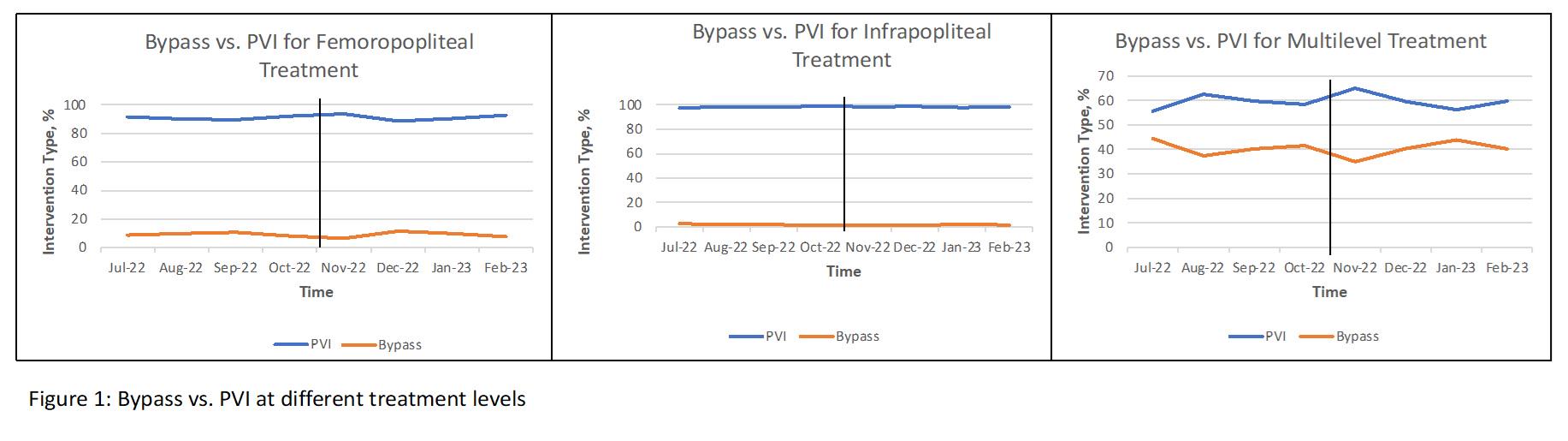
METHODS:The VQI database was used to identify patients with CLTI who underwent either peripheral vascular intervention (PVI) or infrainguinal bypass for infrainguinal revascularization from July 2022 to February 2023 (4 months pre and post BEST-CLI study). Trends in the proportions of PVI or bypass over time were analyzed using Chi-squared trend test, stratified by gender, disease severity (rest pain vs tissue loss), and disease extent (femoropopliteal, infrapopliteal, or multilevel treatment). Bypass patients were further stratified by graft or vein type used and PVI was further stratified by TASC classification.
RESULTS:A total of 174,258 patients were identified (21% bypass). No significant change over time was noted in the proportion of bypass procedures (16% to 14%;p=0.46). Similarly, the bypass proportion remained constant over time in males (17% to 15%;p=0.674) and females (15 % to 14%;p= 0.0947), and in femoropopliteal (8.6% to 7.4%;p=0.383)(Figure 1), infrapopliteal (2.6 % to 1.5%;p=0.907)(Figure 1), and multilevel treatment (44% to 40%; p=0.582)(Figure 1). No significant trends were seen after stratification by vein type for bypass (p=0.865), or by TASC classification for PVI (p= 0.875). The proportion of PVI was higher than bypass overall (21%) but bypass surgery was more common for patients with multilevel disease (52%).
CONCLUSIONS:In the period immediately following BEST-CLI study publication in November 2022, there was no significant change in CLTI treatment preferences. Dissemination of BEST-CLI results is needed to affect current practices. This could be explained due to uncertainty of practicing physicians regarding the generalizability of the trial results considering the exclusion criteria for participants and/or the alarmingly low PVI technical success rate as reported in the trial. It is possible that changes may not be observable yet, so this analysis will be updated once more data is available.

Back to 2024 Display Posters