Back to 2024 Display Posters
Impact Of Community Distress, Gender And Ethnicity Related On Amputation Outcomes After Superficial Femoral Artery Stenting
Antonio Solano, MD, Alejandro Pizano, MD, Michael C. Siah, MD, Gerardo Gonzalez-Guardiola, MD, Khalil Chamseddin, MD, Michael Shih, MD, Vivek Prakash, MD, Shadman Baig, MD, Carlos H. Timaran, MD, Melissa L. Kirkwood, MD.
University of Texas Southwestern Medical Center, Dallas, TX, USA.
OBJECTIVES: We have previously presented that patients treated with superficial femoral artery (SFA) stenting have better outcomes when scheduled duplex surveillance and routine clinical follow-up occurs with reintervention performed for in-stent restenosis (ISR). The relationship between community factors and outcomes after SFA stenting is unknown. We aimed to evaluate the effects of the Distressed Community Index (DCI) and related social parameters on amputation rates after SFA stenting in patients with peripheral arterial disease.
METHODS: Retrospective study of prospectively collected data of patients who underwent SFA stenting between 2005 and 2020 with follow-up at a university hospital. Socioeconomic, demographic, clinical, and imaging information were recorded. Two groups were identified according to zip code level for DCI, which corresponded to more affluent (DCI 1-3) and more disadvantaged (DCI 4-5) communities, respectively. Clinical information included ISR on duplex ultrasound, reintervention, and symptomatic status. The primary endpoint was amputation-free survival, and the secondary endpoints were patency, reintervention, and mortality. Cox multivariate regression and Kaplan-Meier plots were used.
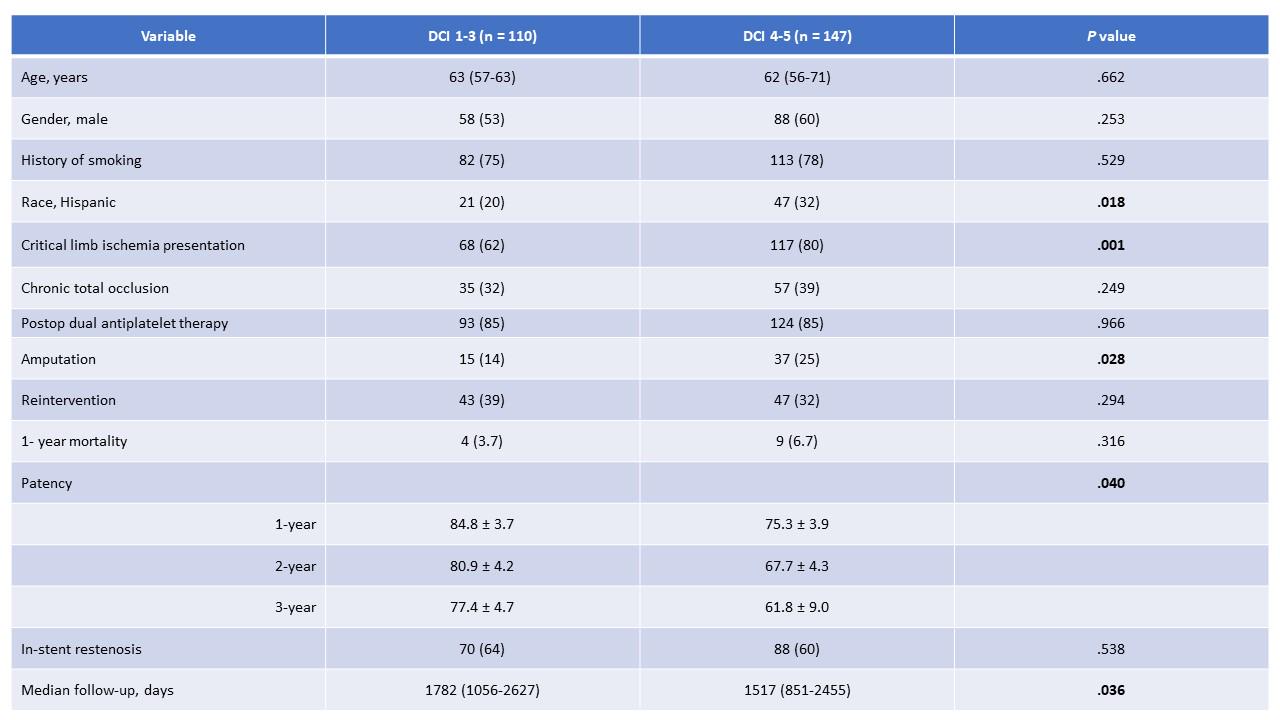
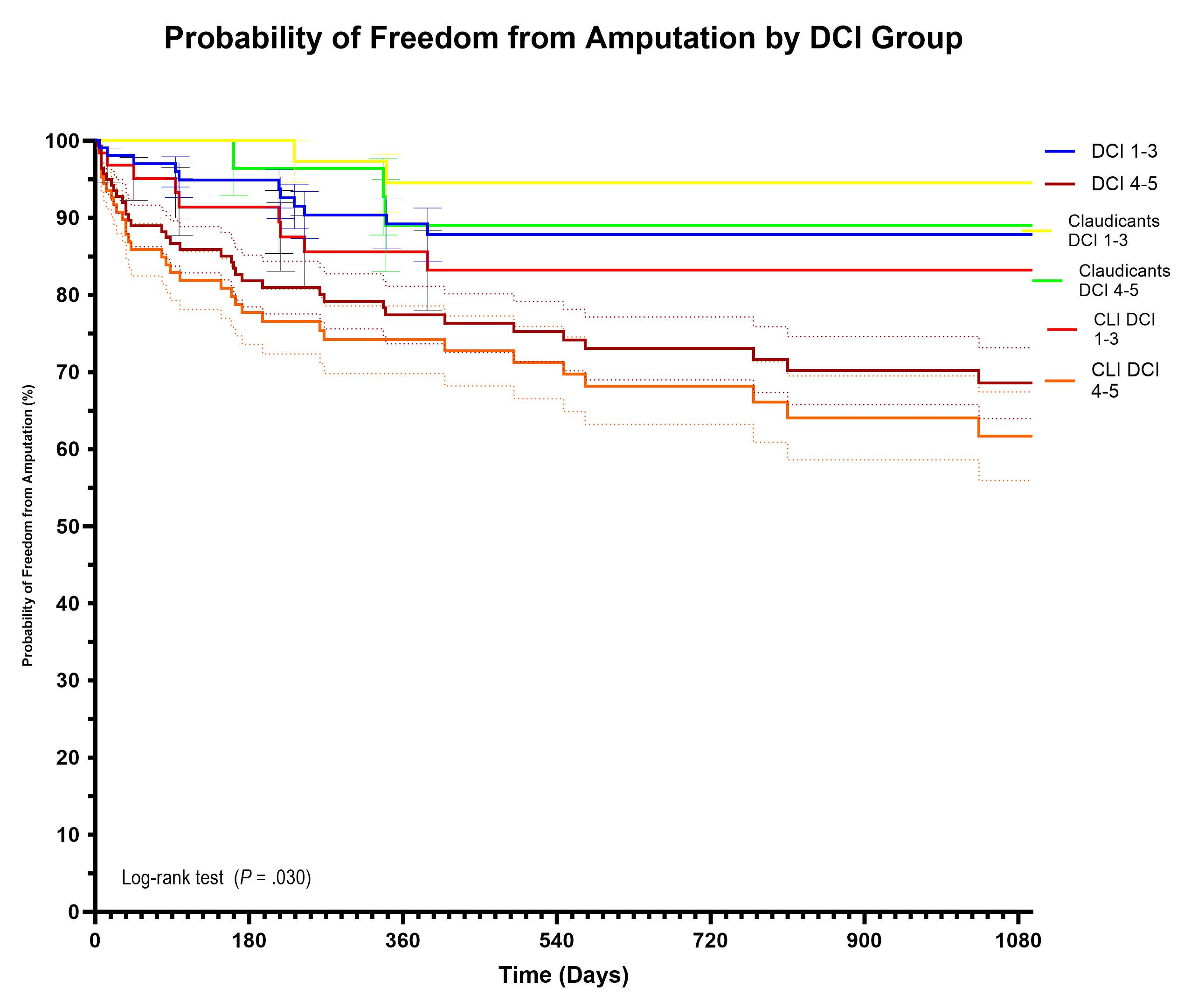
RESULTS: A total of 257 patients were identified, Table 1 depicts the main characteristics of the cohort. The percentage of patients with chronic limb-threatening ischemia was higher for DCI 4-5 (P=.001). Figure 1 demonstrates the probability of amputation-free survival. DCI 4-5 had worse outcomes than patients with DCI 1-3, with no differences for ethnicity or gender. Mortality was lower for DCI 1-3 compared to DCI 4-5 (14% vs 25%, P=.045), with no difference in reintervention. Patients with DCI 1-3 showed higher follow-up rates than DCI 4-5 (P=.036). Adjusted by chronic limb-threatening ischemia, the 2-year freedom of amputation rates were 83.2±5.2 (DCI 1-3) vs. 68.2±5.0 (DCI 4-5); P=.029.
CONCLUSIONS: Patients with a DCI 4-5 were associated with higher amputation and mortality rates than patients with a lower DCI after SFA stenting. This patient population is vulnerable to becoming lost to follow-up, therefore increased physician efforts to maintain active surveillance with prompt intervention for ISR should be emphasized to help ensure long-term limb salvage.


Back to 2024 Display Posters