Back to 2024 Display Posters
The Utility Of Small Artery Disease (SAD) And Medial Arterial Calcification (MAC) Scores In Chronic Wound And Amputation Healing: Can It Tell Us More?
Saranya Sundaram, MD, Christian Barksdale, Stephanie Rodriguez, MD, Mathew Wooster.
Medical University of South Carolina, Charleston, SC, USA.
Introduction: In 2021,Ferraresi et al. described the progressive impact of small artery disease(SAD)and medial arterial calcification(MAC)on wound healing and major adverse limb events(MALE). Their novel scoring system offered data similar to WIfI scoring without significant expertise/cost required. Despite its potential,no subsequent studies have expanded on these findings.We hoped to clarify the clinical utility of SAD/MAC scores in chronic limb threatening ischemia(CLTI)and diabetic wound care.
Methods: Our retrospective review focused on amputations for chronic podiatric wounds(2015-2020)with foot x-ray(MAC)or angiogram(SAD)performed within 6months. Studied outcomes included 1-year healing, amputation,MALE,and amputation-free survival(AFS). Statistics include chi-square,one-way ANOVA, parametric/non-parametric correlation, and Kaplan-Meier analysis.
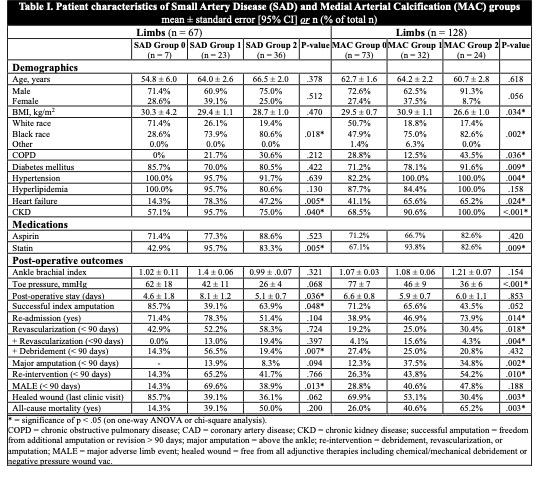
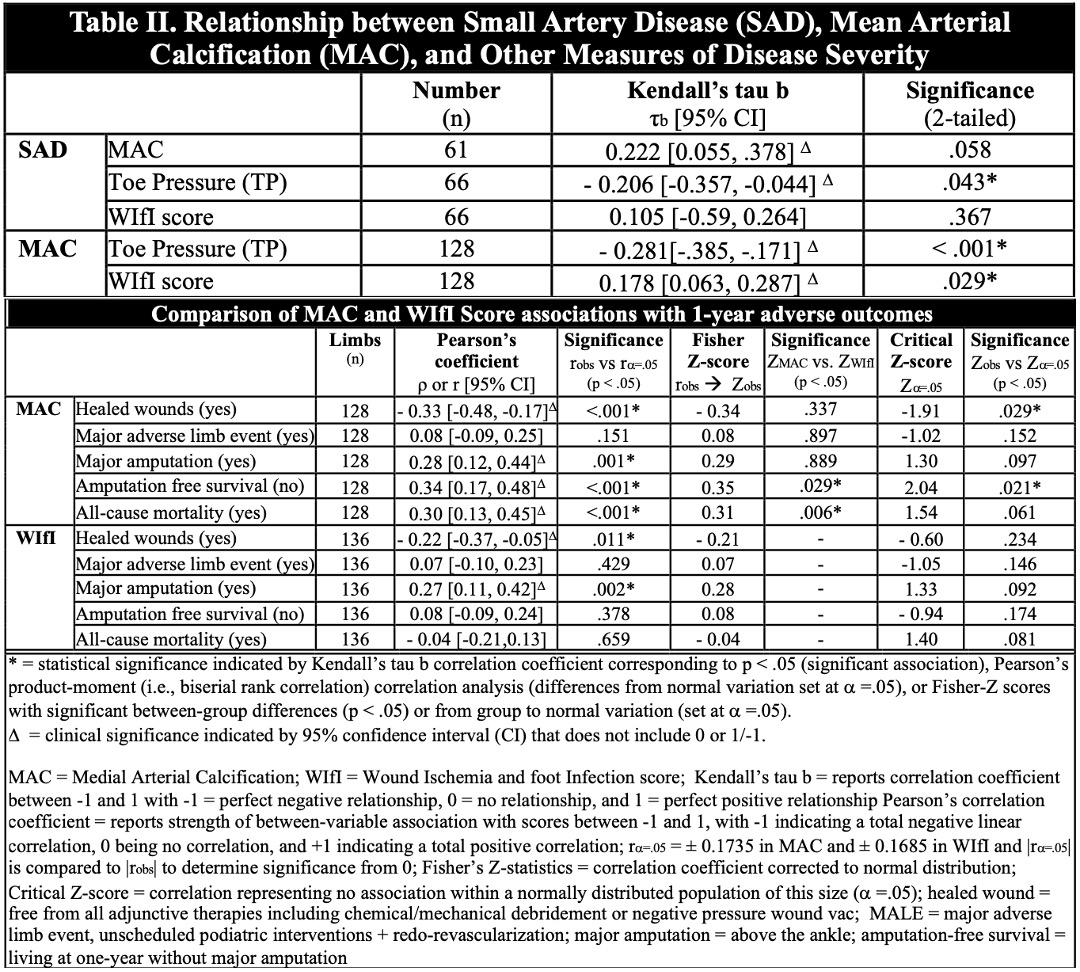
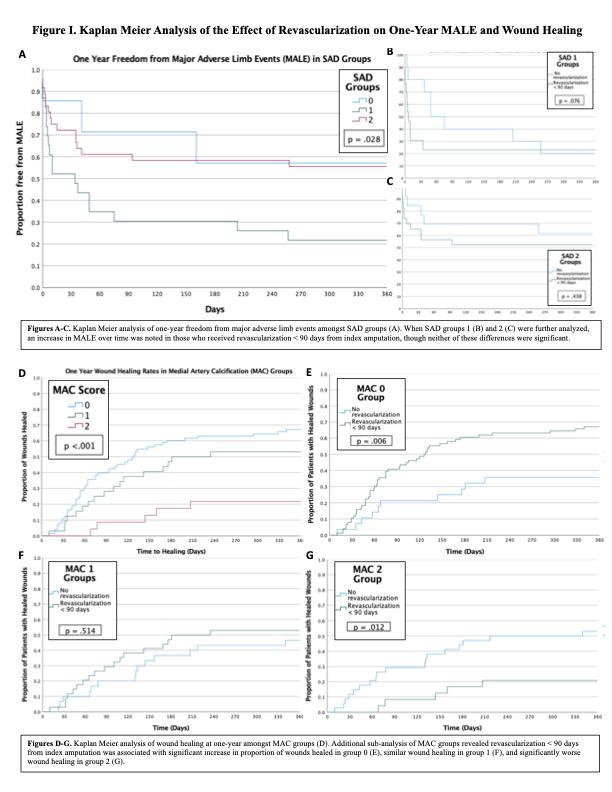
Results: Of 117 patients with 136 limbs,67 could be scored for SAD(0-2)and 128 for MAC(0-2). Cohorts exhibited similar demographics with exception of race,renal disease, diabetes,COPD, hypertension,and heart failure(Table I).High SAD/MAC scores indicated significant below-ankle disease (p =.025[SAD-2],p=.001[MAC-2]) and lower toe pressures (p=.043[SAD],p<.001[MAC],Table-II). Interesingly, SAD-1 patients had higher amputation failure(p=.048), subsequent debridement(p<.007),and one-year MALE(p=.028,Figure-I).Though not significant,Kaplan-Meier analysis demonstrated increased MALE with revascularization<90days in all SAD groups. MAC scores demonstrated stronger,more linear outcome relationships; higher re-admission(p=.014),re-intervention<90 days(p=.010),major amputation<90days(p=.028),and fewer healed wounds(p=.028,Figure II) as MAC increased. Kaplan-Meier analysis suggested revascularization<90days could improve healing in MAC-0(p=.002) with less benefit in MAC-2(p=.012).In our study population, MAC had a significant relationship with wound healing(p=<.001,Table II),major amputation(p=.001),loss of AFS(p<.001),and mortality(p<.001); in comparison,WIfI was only significantly correlated with wound healing(p=.011)and major amputation(p=.002). After adjusting to normal distribution, only relationships between MAC and wound healing(p=.021)or AFS(p=.029)remained significant. Additionally, MAC demonstrated stronger relationships with AFS(p=.029)and all-cause mortality(p=.006) compared to WIfI.
Conclusions: The MAC component of SAD/MAC scoring offers information on wound healing that complements,if not improves upon measures such as WIfI classification. Requiring only a foot x-ray,scores are easy to obtain and perform for any practitioner. Further investigation can delineate the role of this tool as an adjunct to current practice.



Back to 2024 Display Posters