Back to 2024 Display Posters
The Impact Of Gender On Atherectomy Outcomes For Different Anatomic Regions
Andrew Min, BSE, Halbert Bai, MPH, Ajit Rao, MD, Daniel Han, MD, Rami Tadros, MD, Windsor Ting, MD, Christopher Faries, MD, Peter Faries, MD, Ageliki Vouyouka, MD.
Icahn School of Medicine at Mount Sinai, New York, NY, USA.
OBJECTIVES: There is a paucity of research that examines the influence of sex on outcomes after atherectomy for peripheral arterial disease (PAD). This study examines the impact of sex on atherectomy outcomes for different anatomic regions.
METHODS: All patients in the Vascular Quality Initiative (2010-2022) receiving atherectomy were identified. Atherectomy location was stratified into three categories: femoral-popliteal lesions, tibial lesions, and combined infrainguinal lesions. Multivariate logistic regression calculated the odds ratio for various 1-year outcomes, controlling for demographics, clinical presentation, and comorbidities. Kaplan-Meier curves were used to analyze time-to-event data.
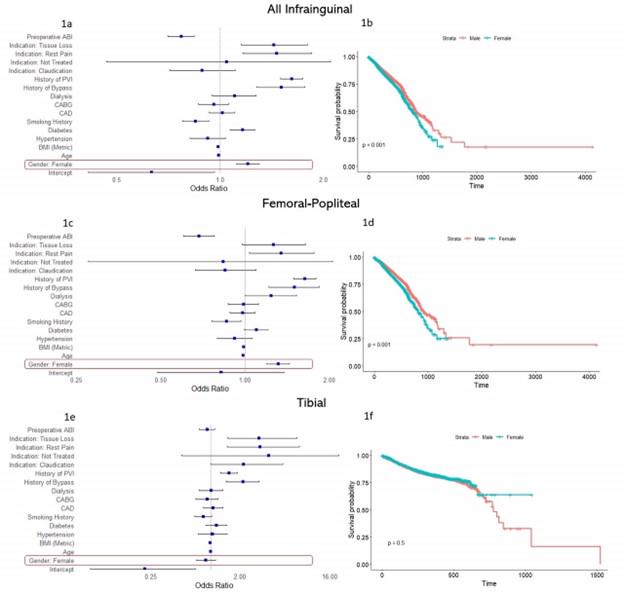
RESULTS: Of the 51,174 combined infrainguinal atherectomy patients, 20,132 (39.3%) were female. Females were more likely to be older (70.8 vs. 69.0, p<0.001), black (21% vs 16%, p<0.001), and present with critical limb-threatening ischemia (52% vs. 49%, p<0.001) and lower ABIs (0.72 vs. 0.81, p<0.001). Females were less likely to be treated for tibial lesions (8.7% vs 16%, p<0.001). For all lesions, females were not more likely to have bail-out stenting after atherectomy (2.5% vs. 2.3%, p=0.11), but were more likely to experience a postoperative complication (10% vs. 8.1%, p<0.001) and a higher odds ratio of 1-year reintervention (OR=1.20, CI=[1.11-1.30], p<0.001). In subgroup analysis, similar trends for early and 1-year outcomes were found for femoral-popliteal lesions, but no sex-related differences were observed for tibial lesions. Interestingly, women were also more likely to have 1-year surgical reintervention after failed atherectomy for femoral-popliteal lesions (OR=1.30, CI=[1.06-1.60], p=0.013) but not tibial lesions (OR=0.82, CI=[0.43-1.48], p=0.5). There was no sex-related difference in major amputation risk between any of the groups. Forest plots and Kaplan-Meier curves for each anatomic subset are shown in Figures 1a-1f.
CONCLUSIONS: Women were more likely to be treated for CLTI, whereas men were more likely to be treated for tibial lesions. Similarly, we found similar 1 year limb salvage for both men and women after atherectomy; however, women are at higher risk of early postoperative complications and higher odds ratio for 1-year reintervention for non-tibial lesions. Further studies focused on specific demographics, risk factors and comorbidities may help us choose the best endovascular approach for different clinical scenarios of PAD.

Back to 2024 Display Posters