Back to 2024 Display Posters
Antiplatelet Therapy Is Associated With Increased Survival And Decreased Reintervention Following Elective Complex Endovascular Repairs
James M. Dittman, MD1, Alexandra Phocas, MD
1, Thomas F. O'Donnell, MD
2, Marc L. Schermerhorn, MD
3, Sara L. Zettervall, MD
1, Kirsten D. Dansey, MD
1.
1University of Washington, Seattle, WA, USA,
2Columbia University Irving Medical Center, New York City, NY, USA,
3Beth Israel Deaconess Medical Center, Boston, MA, USA.
Objectives: Antiplatelet regimens are often prescribed to maintain visceral & renal artery stent patency after complex endovascular aortic repair. Current practice patterns are heterogeneous. We sought to characterize national trends & determine whether antiplatelet regimens independently influence repair outcomes.
Methods: All elective complex endovascular repairs in VQI from 2012-2021 were compiled. Perioperative factors & outcomes were compared by antiplatelet (AP) regimen: dual therapy (D/DAPT), monotherapy (M), & none (N), with patients discharged on anticoagulation (AC) assessed separately from those not on AC. Univariate & multivariate analyses were applied to assess outcomes differences.
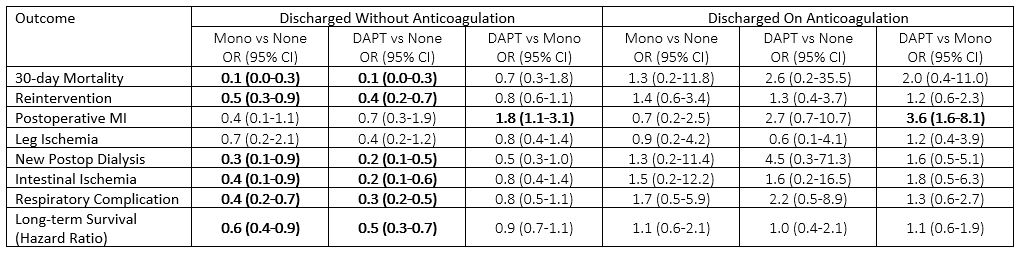
Results: 4,772 patients underwent repair & were discharged on the following regimens: 4% no AP or AC, 34% monotherapy AP without AC, 46% DAPT without AC, 2% AC without AP, 11% monotherapy AP with AC, & 3% on triple therapy.For patients not on anticoagulation, incidence of 30-day mortality (N:6% vs M:1% vs D:1%, p<0.01), reintervention (N:10% vs M:5% vs D:4%, p<0.01), myocardial infarction (N:3% vs M:1% vs D:3%, p<0.01), new postop dialysis (N:3% vs M:1% vs D:1%, p<0.01) & respiratory complications (N:9% vs M:3% vs D:2%, p<0.01) differed by regimen. After adjustment, increased survival was associated with both monotherapy & DAPT compared to no regimen (M HR:0.6; CI:0.4-0.9; D HR:0.5, CI:0.3-0.7) & decreased reintervention (M OR:0.5, CI:0.3-0.9; D OR:0.4, CI:0.2-0.7) (Figure). Of those on anticoagulation, only MI incidence differed by antiplatelet regimen (N:3% vs M:3% vs D:11%, p<0.01), remaining significant after adjustment (Figure).
Conclusions: Antiplatelet therapy should be prescribed to all patients with vascular disease. Antiplatelet regimens were associated with increased survival & decreased reintervention. This medical optimization may be a marker for centers of excellence. More research is needed to determine the optimal regimen for patients on anticoagulation.

Back to 2024 Display Posters