Back to 2024 Display Posters
Hybrid Repair Of Type B Aortic Dissection Involving Aberrant Right Subclavian Artery And Kommerell’s Diverticulum Using A Thoracic Branched Endoprosthesis
Mabel Chan, MD, Sadia Ilyas, MD, Krystal C. Maloni, MD, Steven Abramowitz, MD, Javairiah Fatima, MD.
Medstar Washington Hospital Center, Washington, DC, USA.
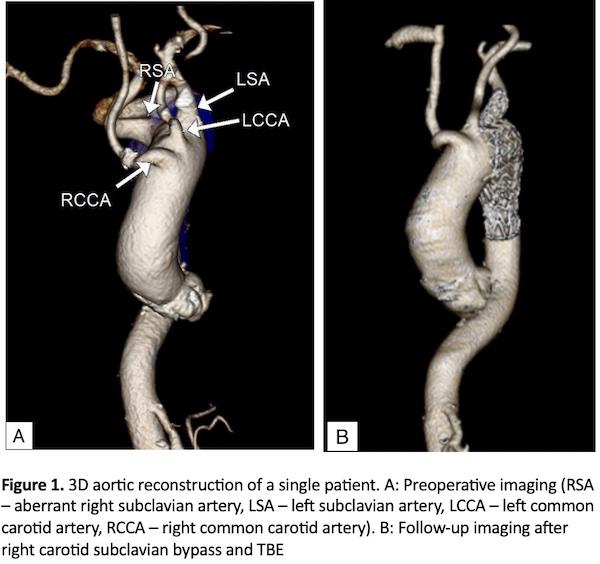
Objective: Aberrant subclavian artery is a commonly described aortic arch branch anomaly that occurs approximately in 0.5% - 1.0% of the population. This can be associated with Kommerell’s diverticulum (KD) and potentially complicated by type B aortic dissection (TBAD) at its ostium (Fig 1A). Traditionally, KD with dissection is treated with open repair; however, favorable outcomes have recently been reported using hybrid, staged approach such as bilateral carotid-subclavian artery bypasses followed by TEVAR. Herein, we report a case series of four patients with KD treated via a hybrid repair with a novel commercially available thoracic branched endograft (Thoracic Branch Endoprosthesis [TBE], WL Gore, Flagstaff, AZ) and single sided surgical revascularization.
Methods: Centerline reconstruction was used for anatomic assessment and operative planning. The patients underwent hybrid endovascular repair incorporating right sided carotid-subclavian bypass (CSB) and TBE placement with the single side branch to the left subclavian artery with proximal landing in zone 1, followed by Amplatzer plug occlusion distal to the KD. Procedure feasibility, patient survival, clinical outcome, and symptom resolution were evaluated. Patients were followed up in clinic with computed tomography angiography (CTA).
Results: Four patients met inclusion criteria; all were females with a mean age of 71.5 ± 18.3 years. Three patients were symptomatic at time of presentation with chest or back pain. Three patients underwent successful single-stage right CSB and TBE, with one patient undergoing TBE one day following right CSB. Technical success was 100% with no major adverse events, including stroke, spinal cord ischemia, MI or death. Median hospital stay was 7 (5-21 days). Branch vessel patency was 100% with complete remodeling achieved in three patients at median follow-up of 2.9 (1.6-8.4 months) (Fig 1B). One patient with 9.5cm aneurysmal degeneration underwent a staged F/BEVAR during index hospitalization to achieve false lumen thrombosis.
Conclusion: TBE with right subclavian artery revascularization is feasible with technical and procedural success and minimal morbidity in patients with aortic dissection in the setting of KD. Future studies and long-term outcomes comparing hybrid approach using TBE device to those with open surgery or TEVAR with bilateral revascularization are warranted.

Back to 2024 Display Posters