Back to 2024 Display Posters
Arterial Duplex Values Differ Among Renal Angiography Patients With And Without Revascularization Whereas Comorbidities And Demographics Did Not Impact Outcomes
Melissa M. D'Andrea, Daniel Nguyen, Reynaldo D. Contreras, Martina Francis, Dylan Joule.
University of Arizona Tucson, Tucson, AZ, USA.
OBJECTIVES: The purpose of this study is to validate renal artery stenosis (RAS) duplex criteria and impact of gender, native vs. transplant renal artery, and other comorbidities on renal artery angiography (RAA) outcomes to potentially reduce the incidence of diagnostically unimpressive angiograms. We sought to validate the currently standardized duplex criteria in combination with risk factors to justify revascularization outcomes at our institution.
METHODS: Patients with RAS undergoing RAA at a single center academic institution between January 2019 through March 2023 were retrospectively reviewed. Duplex-derived PSVs were obtained and compared to whether RAA required balloon angioplasty and/or stenting, or was solely diagnostic. Diagnostic and interventional groups were additionally compared with regards to demographics and risk factors. Unpaired t-test statistical analysis was performed.
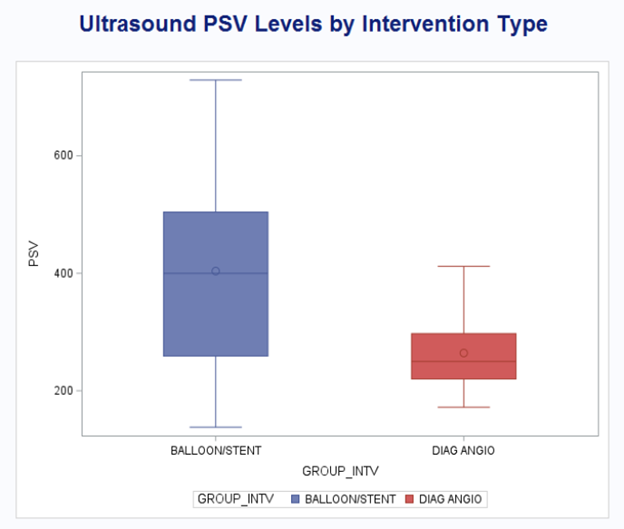
RESULTS: Forty-two patients (21 males, 21 females, mean age 64.02) underwent RAA.. Among them, 13 were excluded either for RAS defined by imaging means other than CDUS, or their duplex findings did not include PSV values due to technical challenges. Of the remaining 29 cases, resulted in diagnostically unimpressive RAAs not requiring intervention, 20 instances of balloon angioplasty and 9 of stenting. The mean PSV of 264.3 cm/s for diagnostic-only RAAs was significantly lower than the mean PSV of 403.8 cm/s for RAAs resulting in balloon angioplasty and/or stenting (p=0.0026). Factors of gender, hyperlipidemia, diabetes mellitus, coronary artery disease, peripheral artery disease, smoking, vasculitis, congenital renal disorder, or history of kidney transplant were not significant predicators for either diagnostic-only or interventional RAAs.
CONCLUSIONS: The mean duplex PSV was significantly higher in patients with balloon angioplasty and/or stenting procedures as compared to patients with diagnostic-only RAAs. A PSV of 264.3 cm/s or below may represent a duplex-defined RAS cutoff to minimize diagnostically unimpressive RAAs, with 411.9 cm/s potentially serving as an upper threshold above which adjunctive intervention is significantly more likely to be performed. Gender and other comorbidities did not affect intervention outcomes. Larger scale studies from multiple sites and randomized control studies are needed to investigate predictors for need for intervention. Thorough sensitivity/specificity analysis, is required to better define a more optimal interventional threshold.

Back to 2024 Display Posters