OBJECTIVE: National guidelines recommend long-term surveillance after endovascular AAA repair (EVAR) to monitor for endoleaks, graft migration or device failure. However, multiple investigations have demonstrated that EVAR follow-up can vary greatly. Recently, the Blue Cross Blue Shield of Michigan Cardiovascular Consortium (BMC2) implemented a performance metric, linked with financial reimbursement, designed to improved EVAR postoperative surveillance. The purpose of this study was to evaluate the impact of this statewide incentive metric on EVAR follow-up and long-term endovascular outcomes.
METHODS: The BMC2 statewide cardiovascular consortium consisting of 36 hospitals was queried for patients who underwent EVAR between 2017-2021. Patient, hospital and operative risk factors were collected and analyzed based on the presence or absence of 1-year follow-up EVAR surveillance imaging. The primary outcome was adherence to recommended EVAR surveillance and the longitudinal change in percent of EVARs that obtained surveillance imaging by hospital during the study period.
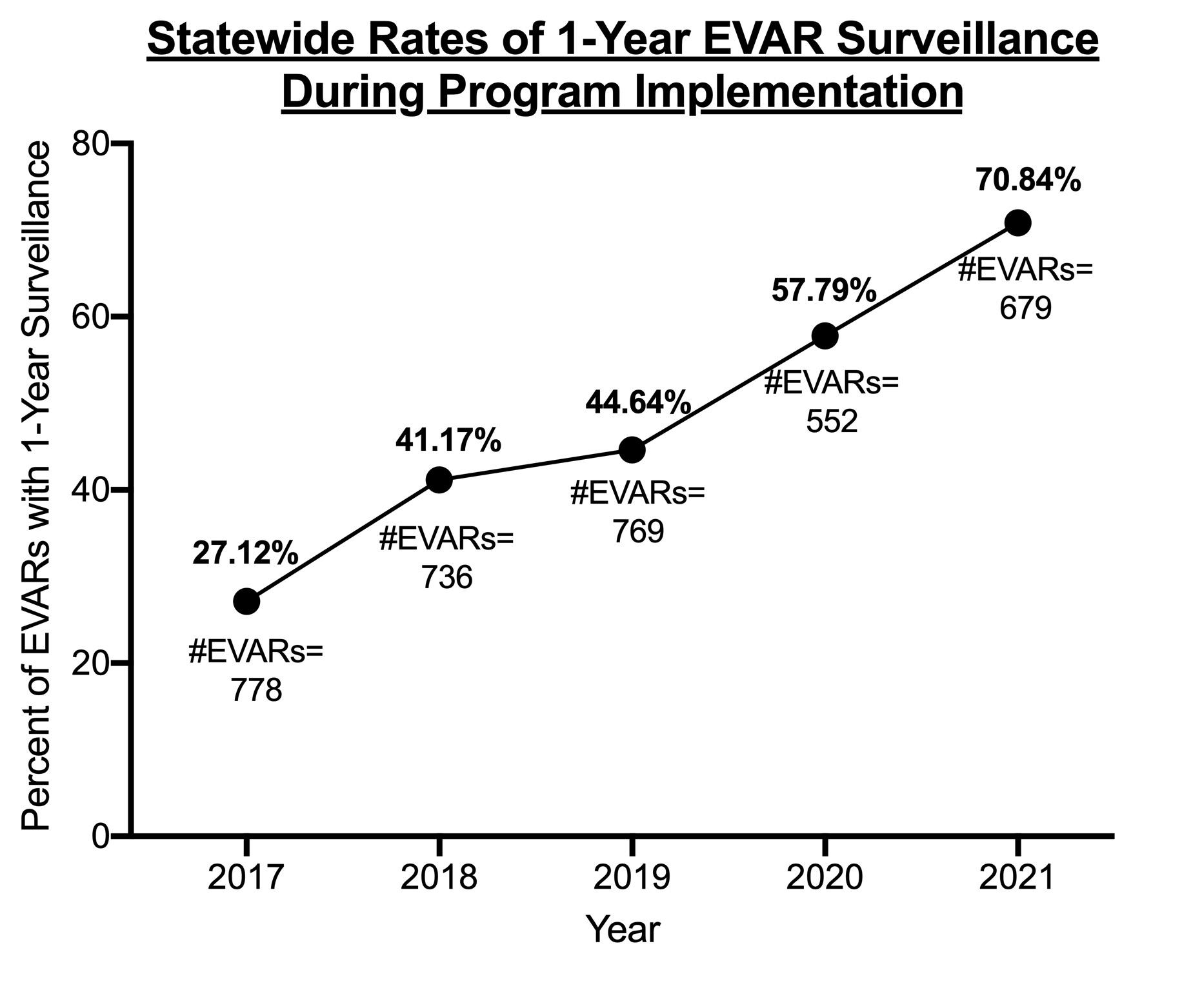
RESULTS: A total of 3,435 patients underwent EVAR between 2017-2021. During the implementation of the EVAR surveillance metric, there was steady increase in the annual percentage of EVARs across the state who received postoperative surveillance imaging (27.1% in 2017 increasing to 70.8% in 2021). At the hospital level, the average change in the percentage of EVARs with documented 1-year surveillance was +46.9%±5.5% per hospital over the study period. On univariable analysis, patients without EVAR follow-up had worse baseline functional status and more comorbidities including COPD and valvular disease. Following mixed logistic modeling, patients that received EVAR follow-up had a significantly higher number of repeat interventions (3.2% vs.1.8%; p<0.01) but were found to have significant decrease in one-year mortality (0.7% vs 12%; p<0.01) compared to those did not receive one-year EVAR surveillance.
CONCLUSIONS: Incomplete imaging surveillance following EVAR remains high and predisposes patients to worse survival outcomes. Utilization of a performance metric, and associated financial incentive, within a statewide quality collaborative is a viable strategy that can have a significant impact on increasing EVAR surveillance and decreasing long-term mortality after endovascular repair.