Back to 2024 Karmody Posters
A Transcarotid Artery Revascularization (TCAR)-first Approach In Patients Requiring Surgery For Cervical Carotid Disease
Shin Mei Chan1, Julia F. Chen, M.D.
2, Nupur Nagarkatti, M.D.
3, Sarah Loh, MD
3, Britt Tonnessen, MD
3, Uwe Fischer, MD
3, Naiem Nassiri, MD
3.
1University of California, San Francisco, San Francisco, CA, USA,
2University of Toronto, Toronto, ON, Canada,
3Yale University School of Medicine, New Haven, CT, USA.
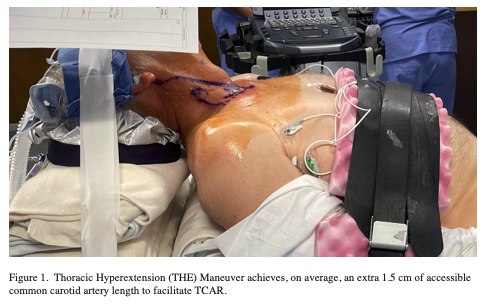
OBJECTVES: Transcarotid artery revascularization (TCAR) has evolved into a viable surgical alternative in high-risk carotid endarterectomy (CEA) patients. Despite recent FDA approval for standard-risk patients, its role as first-line surgical option for cervical carotid disease remains unknown. We present our experience with a TCAR-first approach. METHODS: From 2020-2023, consecutive patients with symptomatic / asymptomatic cervical carotid disease meeting criteria for surgical intervention were treated with a TCAR-first approach by a single operator. CEA or transfemoral stenting (TFS) were offered to patients who did not meet anatomic criteria for TCAR based on instructions for use (IFU). TCAR was offered outside IFU later in the experience in select patients with employment of operative / non-operative adjunctive maneuvers. Best medical therapy were routinely employed. Data was prospectively maintained and retrospectively reviewed for a primary composite end point of stroke, MI, and death within 30 days; and secondary end-points of ipsilateral stroke beyond 30 days and post-operative complications. RESULTS: 139 patients underwent treatment with TCAR-first approach. TCAR was performed in 119 (86%) patients (mean age 73, range 54-88 years; 96% male; 27% symptomatic; 90% high surgical risk). The remaining 20 underwent CEA (n=18; 13%) or TFS (n=2; 1.4%). The primary composite endpoint of stroke, MI, and death with TCAR at 30-days was 0. Incidence of ipsilateral stroke beyond 30 days after TCAR was 0 (mean follow-up of 14.5 months, range 1 - 50 months). TCAR complications were limited to 4 (3.3%) incisional infection cases, 2 (1.6%) of which required surgical incision / drainage; and 2 (1.6%) case of transient hoarseness. In 32 (27%), TCAR was performed outside the IFU due to short (< 5 cm) CCA length initially by surgical conduit creation in 2 (1.6%) patients, and later by a surgeon-devised thoracic hyperextension (THE) maneuver (n=30; 25%) with an average accessible CCA length gain of 1.5 cm (0.5 - 3 cm) (Figure I). CONCLUSIONS: TCAR is a safe and effective first-line surgical option in high- and standard-risk patients with symptomatic / asymptomatic cervical carotid disease. Certain anatomical barriers to TCAR can be safely overcome by operative / non-operative maneuvers.

Back to 2024 Karmody Posters