Back to 2024 Karmody Posters
Does Anesthetic-modality Affect Post-operative Amputation Outcomes
Nakia Sarad, DO1, Sophie Kush, BS
1, Rowza Rumma, MD
1, Angelina Kim, MD
2, Nitin Jethmalani, MD
1, Zoe Verzani, MPH
1, Rajeev Dayal, MD
2, Varuna Sundaram, MD
2, Andy Lee, MD
2, Jing Li, MD
2, Christopher Agrusa, MD
1, Sharif Ellozy, MD
1, Brian DeRubertis, MD
1, Peter Connolly, MD
1.
1Weill Cornell Medical Center, New York, NY, USA,
2New York-Presbyterian/Queens, Flushing, NY, USA.
OBJECTIVES: General anesthesia (GA) is recognized to carry significant cardiopulmonary and stroke risks, especially amongst the peripheral arterial disease patient population. Although regional anesthesia (RA) has been considered as an anesthetic alternative for lower extremity amputations (LEA), only 15% of all LEAs utilize RA and there are inconsistent post-operative outcome findings across studies. Our institution has adopted RA into routine use, and so our study aims to investigate the clinical outcomes of anesthetic-modality for non-traumatic proximal LEAs.
METHODS: Through an institutional database, we retrospectively examined all lower extremity amputations between 2017 to 2022. All non-traumatic below-knee (BKA) and above-knee (AKA) amputations were included. Patients were categorized into two cohorts based on anesthetic modality of either GA or RA. RA was considered local or regional block. Basic demographics, comorbidities, and outcomes were collected and analyzed using multivariate regression.
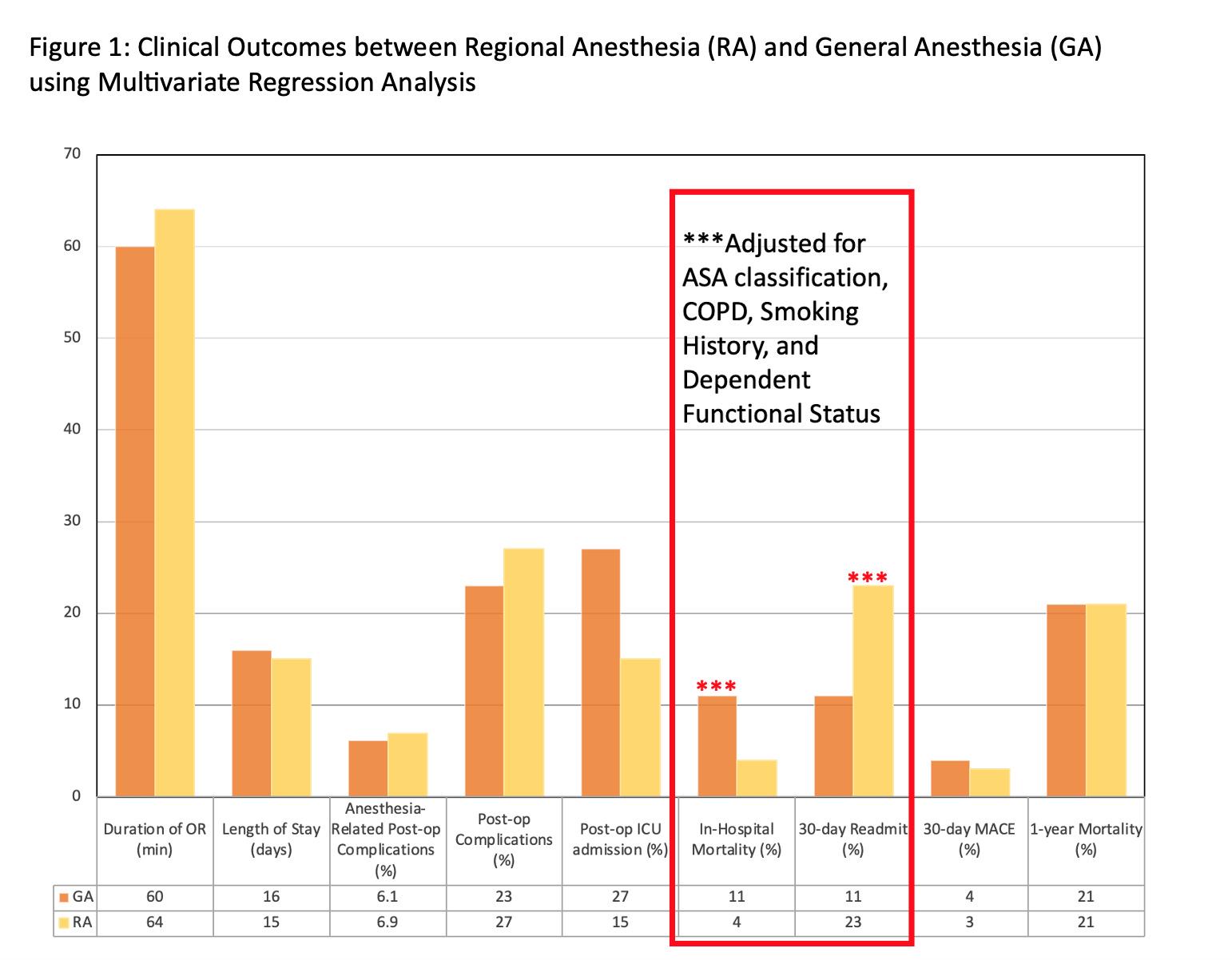
RESULTS: There were 511 amputations during the study period, 34% AKAs(n=172) and 66% BKAs(n=339). Median age of study population was 68(IQR 57,77) with 62% male(n=315). The distribution of anesthetic-modality for LEAs was balanced, 54.4% GA(n=278) and 45.6% RA(n=233). 32% of AKAs(n=54) and 53% of BKAs(n=179) were performed under RA, with higher incidence of BKAs to undergo RA(77% v. 23%,p<0.01). There were no significant differences between age, gender, race, BMI, and residence. More patients with dependent functional status underwent GA than RA(49% v 37%,p<0.01) There was no significant difference in ASA-classification, pre-operative infectious status, or comorbidities between the two cohorts, except higher incidence of COPD and tobacco abuse with GA cases(p<0.05). When adjusting for COPD, tobacco abuse, and dependent functional status, RA was associated with lower in-hospital mortality(3.9% v.11%,OR 0.22,95% CI 0.07-0.56,p<0.01,Figure 1), but associated with higher 30-day readmission rates (23% vs.11%,OR 2.77,95% CI 1.60-5.00,p<0.01). There was no significant difference in operative time, anesthesia-related complication rate, overall complication rate, 30-day major adverse cardiovascular events(MACE), length of stay(LOS), and 1-year mortality.
CONCLUSIONS: Although regional anesthesia has lower in-hospital mortality than general anesthesia, anesthetic-modality does not affect overall post-operative outcomes for morbidity and mortality for PAD patients undergoing proximal amputations. Regional anesthesia is equivocal to and is a safe alternative to general anesthesia for lower extremity amputations.

Back to 2024 Karmody Posters