Back to 2024 Karmody Posters
Contemporary Use Of Suboptimal Great Saphenous Vein In Lower Extremity Bypass Yields Favorable Mid-term Patency
Colin Cleary, PhD1, Ya-Huei Li
2, James Gallagher III
3, Parth Shah
3, Thomas Divinagracia
3, Akhilesh Jain
3, Elizabeth Aitcheson
3, Mouhanad Ayach
3, Owen Glotzer
3, Ryder White
3, Kristy Wrana
3, Edward Gifford
3;
1University of Connecticut School of Medicine, Farmington, CT, USA,
2Hartford HealthCare Research Administration, Hartford, CT, USA,
3Hartford HealthCare Division of Vascular and Endovascular Surgery, Hartford, CT, USA
OBJECTIVES: Historically, studies have identified a great saphenous vein (GSV) diameter of at least 3.0mm for optimal durability following lower extremity bypass. With the recent publication of BEST-CLI and BASIL-2 studies, we sought to compare patency and post-operative complications utilizing GSV conduit of <3.0mm to veins ≥3.0mm or PTFE grafts from a single institution.
METHODS: Patients with pre-operative GSV vein mapping in an Intersocietal Accreditation Commission accredited vascular lab who underwent infra-inguinal bypass surgery at a tertiary center were included. Vascular lab software was utilized to compare patient median GSV across at least six anatomic locations. Patients were seperated and stratified based on median GSV size (both overall and limited to above-knee GSV). Concomitant patients undergoing PTFE bypass were included for comparison. Primary outcomes included post-operative complications, 30-day major adverse limb events (MALE), major adverse cardiac events (MACE), and patency at regular follow-up intervals.
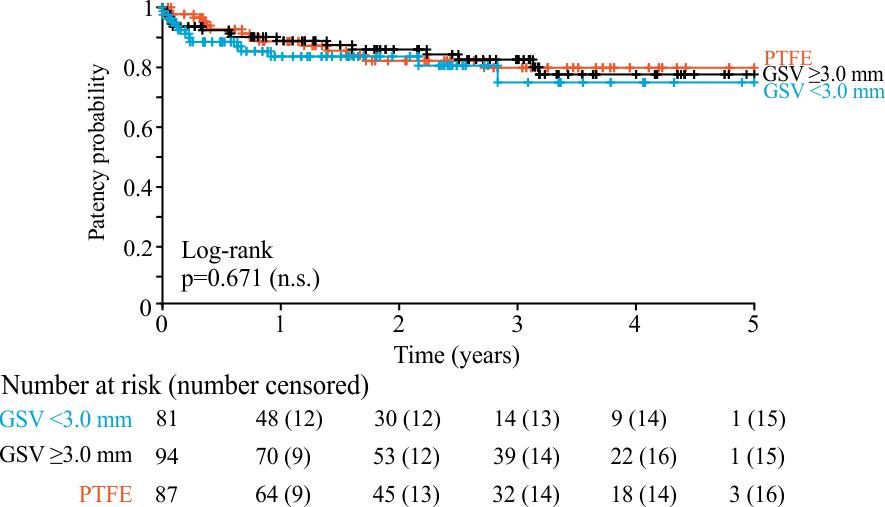
RESULTS: From 1/2016 to 2/2022, 267 patients underwent bypass with pre-operative vein mapping: 89 of which received PTFE, 82 who received GSV<3.0mm, and 96 who received GSV≥3.0mm. Patients were evenly distributed in demographics including age, gender, smoking history, and proximal and distal targets. Median follow-up to 2/2023 was 1.90 years for the combined cohort. Overall, use of <3.0 mm GSV was not associated with inferior primary patency compared to ≥3.0 GSV or PTFE (two-year patency rate: GSV<3.0 mm 83.5%, GSV≥3.0mm 85.8%, PTFE 82.0%;
Figure 1). There were no differences in 30-day MACE between groups, however, there was increased incidence of 30-day MALE in patients receiving GSV<3.0mm compared to GSV≥3.0mm (9.8 vs 2.1%, p=0.030), driven by higher rates of re-intervention to maintain patency without differences in major amputation. Patients who received GSV≥3.0mm (2.7%) had a lower risk of surgical site infection when compared to GSV<3.0mm (13.8%) and PTFE patients (12.0%, p=0.049).
CONCLUSIONS: In our cohort, patients who received GSV bypasses <3.0mm have the same mid-term patency as patients who received GSV≥3.0mm. Use of smaller GSV may require earlier reintervention, and therefore closer follow-up to maintain patency. Nonetheless, under appropriate circumstances, sub-optimal GSV can be utilized for lower extremity arterial bypass.

Back to 2024 Karmody Posters