Back to 2024 Karmody Posters
Outcomes Following Unilateral Axillofemoral Bypass Versus Crossover Femorofemoral Bypass In Chronic Limb Threatening Ischemia Patients
Sai Divya Yadavalli, MD1, Lucas Souza-Mota, MD
1, Winona Wu, MD
1, Vinamr Rastogi, MD
2, Carla Moreira, MD, RPVI
3, Jeffrey Siracuse, MD
4, Marc L. Schermerhorn, MD
1, Lars Stangenberg, MD
1;
1BIDMC, Boston, MA, USA,
2Erasmus University Medical Center, Rotterdam, Netherlands,
3Brown University, Providence, RI, USA,
4Boston University, Boston, MA, USA
Objective: In patients with chronic limb-threatening ischemia (CLTI) with aorto-iliac occlusive disease, extraanatomical bypasses are an alternative in patients who cannot tolerate aortic cross clamping necessary for anatomical reconstruction, or in those with a hostile abdomen. Given their infrequent use, direct comparisons between unilateral axillofemoral bypass (AxFB) versus femoro-femoral bypass (FFB) for CLTI remain scarce. We evaluated postoperative and 5-year outcomes following AxFB versus FFB for CLTI.
Methods: We identified patients undergoing elective/semi-urgent unilateral AxFB and FFB in the VQI linked to Medicare claims between 2014-2019, excluding procedures with concomitant bypasses/interventions. We performed 1:2 (AxFB:FFB) propensity score matching for baseline demographics, comorbidities, urgency, ipsilateral and contralateral presentation (rest pain vs ulcer/gangrene), and prior interventions/bypass procedures. We analyzed perioperative and 5-year outcomes using logistic regression and Cox-regression models.
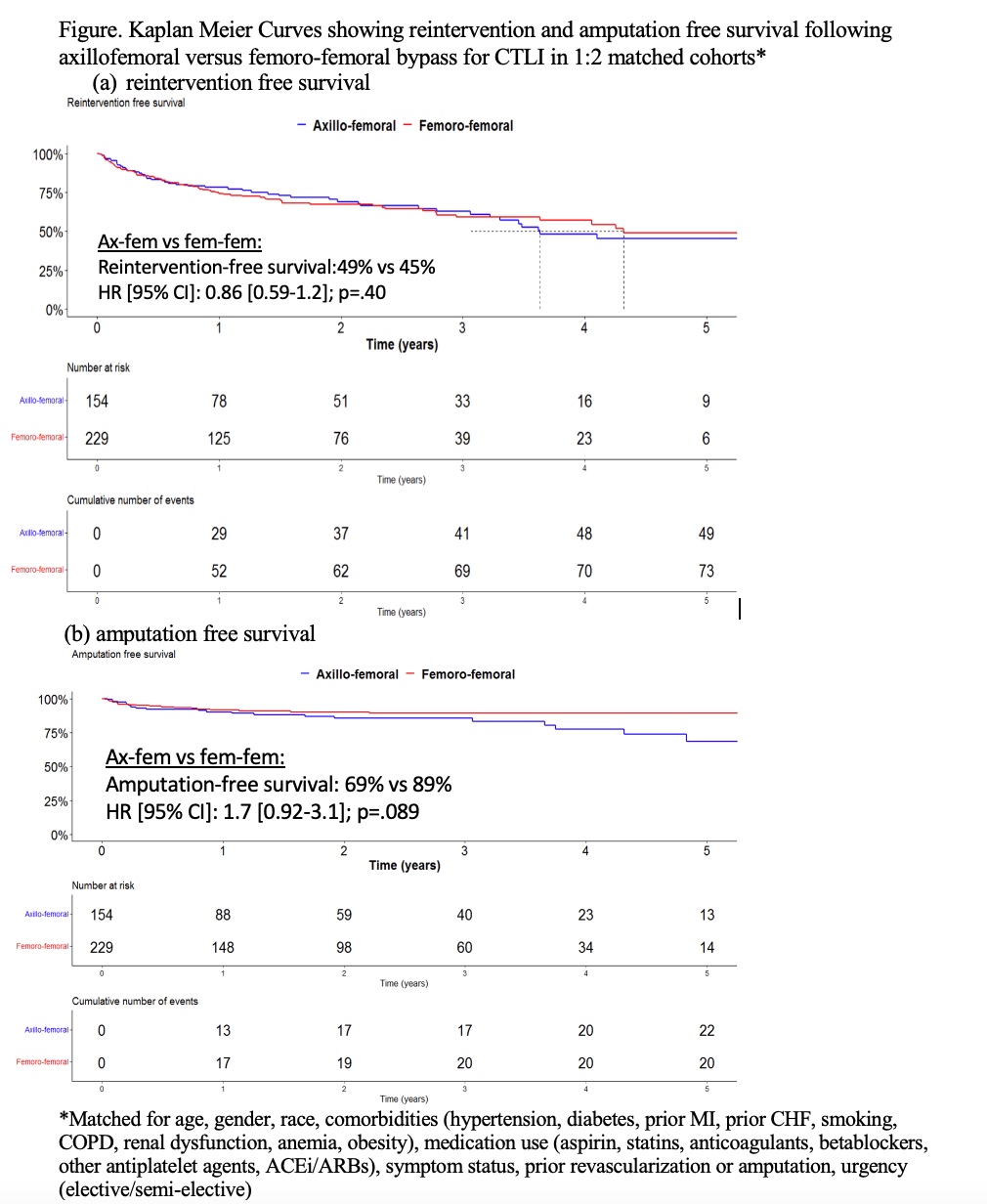
Results: We included 1,185 patients (27% AxFB), of whom 224 AxFBs matched with 374 FFBs. After matching, perioperative mortality was comparable between AxFB and FFB bypass groups (15% vs 10%; p=.12). However, AxFB patients had higher rates of postoperative complications (30% vs 15%;p<.001), specifically ipsilateral amputations (below-knee:1.8% vs 0.5%; above-knee:5.4% vs 2.4%;p=.049), in-hospital reintervention (13% vs 7.2%;p=.040), and wound complications (5.9% vs 1.6%;p=.012). Primary/primary assisted patency at discharge was lower following AxFB (96% vs 98%;p=.018), nevertheless, secondary patency was comparable (1.3% vs 0.6%;p=.25). Postoperative length of stay was higher in the AxFB patients (5 days vs 3 days; p<.001), rates for discharge to home were lower (57% vs 68%;p=.066). At 5-years, AxFB was associated with lower rates of 5-year survival (41% vs 46%; aHR: 1.3[1.0-1.7];p=.046), comparable reintervention free survival (45% vs 49%; aHR: 0.86[0.59-1.2];p=.40 | Figure a) and lower major-amputation free survival (69% vs 89%; aHR: 1.7[0.92-3.1];p=.089 | Figure b).
Conclusion: Unilateral AxFB for CLTI was associated with higher postoperative complications when compared with FFB. Similarly, 5-year results demonstrate higher mortality and lower major amputation-free survival in the AxFB group. Based on our findings, unilateral axillofemoral bypass may be considered second line treatment for the treatment of aorto-iliac occlusive disease in CLTI patients with reasonable short- and long-term outcomes in patients unsuitable for a femorofemoral bypass.

Back to 2024 Karmody Posters