Back to 2024 Karmody Posters
Early Experience With Patient-specific Unibody Bifurcated Fenestrated-branched Devices For Complex Endovascular Aortic Aneurysm Repair
Mira T. Tanenbaum, MD1, Andres V. Figueroa, MD
1, Lucas Kanamori, MD
2, Marilisa Soto Gonzalez, MD
1, Jose Eduardo Costa Filho, MD
1, Titia Sulzer, Bsc
2, Thomas Mesnard, MD
2, Ying Huang, MD, PhD
2, Mirza S. Baig, MD
1, Gustavo S. Oderich, MD
2, Carlos H. Timaran, MD
1;
1University of Texas Southwestern Medical Center, Dallas, TX, USA,
2The University of Texas Health Science Center at Houston, Houston, TX, USA
OBJECTIVES: Short distances between the lowest target vessel and aortic bifurcation are technically challenging during fenestrated-branched endovascular aortic repair (FBEVAR). The use of inverted limb bifurcated devices for FBEVAR is limited by short overlap, difficult cannulation, and potential stent compression. This study reviews the early experience of patient-specific unibody bifurcated FB-devices for FBEVAR.
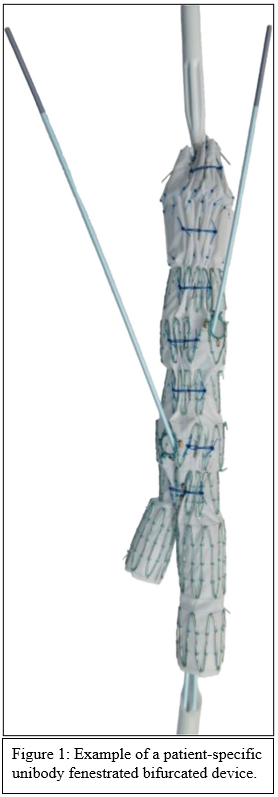
METHODS: Consecutive FBEVAR procedures over a 34-month period with unibody bifurcated FB-devices in physician-sponsored investigational device exemption studies at two institutions were reviewed. Unibody bifurcated FB-designs encompassed fenestrated bifurcated (Fig 1), fenestrated inverted limbs, or bifurcated FB-devices. Endpoints included technical success, survival, frequency of type I or III endoleaks, limb occlusion, and secondary interventions.
RESULTS: Among 168 patients undergoing FBEVAR, 33 (19.6%) patients (78.7% male; mean age 77) received unibody bifurcated FB-devices. Fenestrated bifurcated, fenestrated inverted limb, and bifurcated FB-devices were used in 24 (72.7%), 2 (6.06%), and 7 (21.2%) patients, respectively. Median maximum aneurysm diameter was 61 mm (55-69). Prior endovascular aneurysm repair was reported by 29 (87.9 %) patients; 2 (6.06%) had suprarenal stents. A short distance between the lowest target vessel and aortic bifurcation (mean distance 49.1�4.2 mm) was evident in 30 (90.9%) patients. A total of 128 fenestrations were planned. Preloaded devices were used in 23 patients (69.7%). Median operative time was 238 min (226-300), fluoroscopy time was 65.5 min (56.0-77.7), and dose area product was 147 mGy.cm
2 (105-194). Exclusive femoral access was used in 14 (42.4 %) procedures. Technical success was 100%. Target vessel primary patency was 100% at median follow-up of 11.7 months (3.5-18.6). Two (6.06%) patients required reintervention for iliac occlusion, with one requiring stenting and the other a femoral-femoral bypass. Two (6.06%) patients died from causes unrelated to their aneurysm or repair. During follow-up, 11 (33.3 %) type II endoleaks and one (3.03%) type Ib endoleak were detected; the latter was treated with leg extension. No type I or III endoleaks occurred.
CONCLUSIONS: FBEVAR using unibody bifurcated FB-devices is a safe, feasible and cost-effective treatment option for patients with short distances between the target arteries and aortic bifurcation. Further studies should assess benefits and durability of unibody bifurcated FB-devices.

Back to 2024 Karmody Posters