Back to 2024 Karmody Posters
Earned Outcomes Correlate With Reliability-adjusted Surgical Mortality After Abdominal Aortic Aneurysm Repair And Predict Future Performance
Douglas W. Jones1, Jessica P. Simons
1, Nicholas H. Osborne
2, Marc Schermerhorn
3, Justin B. Dimick
2, Andres Schanzer
1.
1UMass Memorial Medical Center, Worcester, MA, USA,
2University of Michigan, Ann Arbor, MI, USA,
3Beth Israel Deaconess Medical Center, Boston, MA, USA.
OBJECTIVES: Cumulative, probability-based metrics are regularly used to measure quality in professional sports, but these methods have not been applied to health care delivery. We sought to validate a novel measure of surgical quality based on earned outcome methods (deaths above average, DAA) against the current gold standard (reliability-adjusted mortality rates), using abdominal aortic aneurysm (AAA) repair outcomes.
METHODS: Hospital-level DAA were calculated (sum of observed - predicted risk of death for each patient, using established multivariable logistic regression modeling) for elective open AAA repair and EVAR in the VQI (2016-2019). Correlations of DAA with reliability-adjusted mortality rates and procedure volume were determined. 2016-2017 outcomes were used to categorize hospital quality; the ability of these categories to predict 2018-2019 risk-adjusted outcomes was determined.
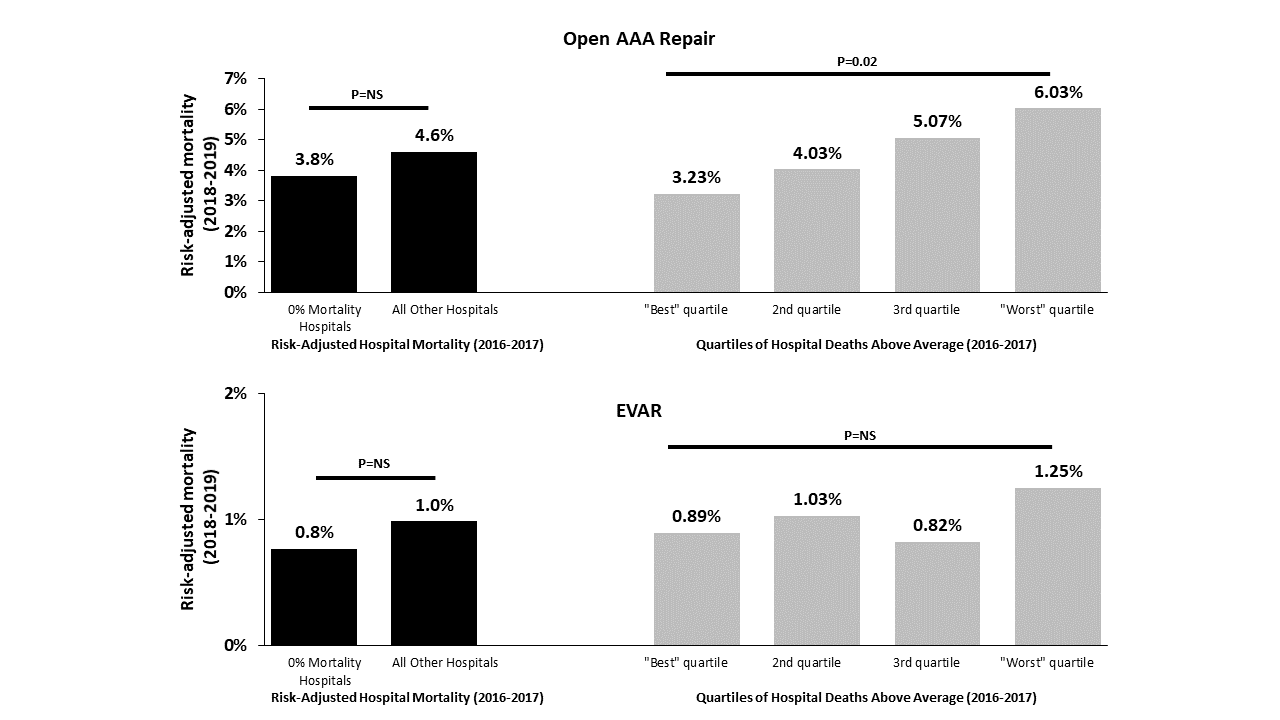
RESULTS: 3,734 patients underwent open repair (106 hospitals), and 20,680 patients underwent EVAR (183 hospitals). DAA was closely correlated with reliability-adjusted mortality rates for open repair (r=0.94, P<0.001) and EVAR (r=0.99, P<0.001). DAA also correlated with hospital volume for open repair (r=-.54, P<0.001), but not EVAR (r=0.07, P=0.3). In 2016-2017, most hospitals had 0% mortality (55% open repair, 57% EVAR), making it impossible to evaluate these hospitals using traditional risk-adjusted mortality rates alone. Further, zero mortality hospitals in 2016-2017 did not demonstrate improved outcomes in 2018-2019 for open repair (3.8% vs 4.6%, P=0.5) or EVAR (0.8% vs 1.0%, P=0.2) compared to all other hospitals. In contrast to traditional risk-adjustment, 2016-2017 DAA evenly divided centers into quality quartiles which predicted future mortality for open repair (Figure). Using 2016-2019 DAA to define quality, highest quartile open repair hospitals had lower median DAA compared to lowest quartile hospitals (-1.18 DAA vs +1.32 DAA, P<0.001), correlating with lower median reliability-adjusted mortality rates (3.6% vs 5.1%, P<0.001).
CONCLUSIONS: Adjustment for differences in hospital volume is essential when measuring hospital-level outcomes. Earned outcomes correlate with reliability-adjustment but are easier to calculate and interpret, and can be utilized when event rates are low. From 2016-2019, highest quality open AAA repair hospitals each prevented >1 perioperative death compared to the average hospital, and >2 perioperative deaths compared to lowest quality hospitals.

Back to 2024 Karmody Posters