Endovascular Revascularization of Femoropopliteal Chronic Total Occlusions versus Stenotic Lesions for Intermittent Claudication: Does the Length of CTO Impact Outcome?
Objective: Endovascular revascularization is generally recommended for short (< 5cm) femoropopliteal chronic total occlusions (CTOs) and increasingly used to treat longer CTOs. However, the long-term outcomes of revascularization of CTOs in comparison to that of stenotic lesions in patients undergoing revascularization for intermittent claudication remain unclear.
Methods: We utilized CPT billing codes to identify lower extremity endovascular revascularizations performed by a single group of surgeons between 2013 and 2023. Chart review then identified for inclusion in the analysis elective procedures that were performed in the femoropopliteal segment for an indication of claudication, had complete angiogram imaging available for review, and had long-term clinical follow up. Only the first revascularization procedure performed in each limb was included. Long term outcomes were compared with Kaplan Meier curves.
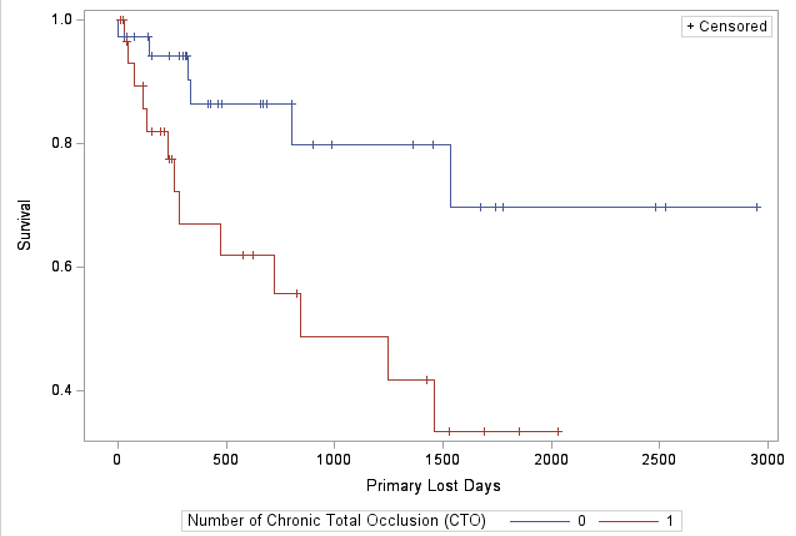
Results: Out of 609 total lower extremity endovascular revascularizations over the study period, 69 met inclusion criteria for this study. 31 patients (46%) had a femoropopliteal CTO while 38 (54%) had stenotic lesions. The median CTO length was 7.7 cm (5-31 cm). Comorbidities and the method of revascularization were not different between the CTO and stenotic group. At a median follow up of 1931 days [IQR 1948 days], revascularization of a CTO was associated with significantly inferior primary (CTO: 65% vs. Stenotic: 85%, Figure), primary assisted (CTO: 65% vs. Stenotic: 95%), and secondary patency (CTO: 77% vs. Stenotic: 95%) in comparison to revascularization of stenotic lesions (log rank test, P< 0.05 for all). Clinically -driven reintervention, major adverse limb events, and overall survival were not different between groups. The outcomes of treatment of short CTOs (<5 cm) were not significantly different than that of longer CTOs (≥5 cm).
Conclusions: In patients with intermittent claudication, endovascular revascularization of a femoropopliteal CTO, irrespective of length, is associated with worse long-term patency than revascularization of a stenotic segment. Additional study on the long-term outcomes of endovascular revascularization of CTOs is necessary to inform recommendations regarding revascularization for intermittent claudication.