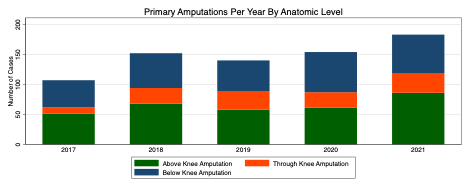
Objective: Single-center civilian series report a 10-30% primary amputation rate following lower-extremity vascular trauma (LEVT). We characterize incidence and identify risk factors for primary amputation after LEVT using the Trauma Quality Improvement Program (TQIP) registry, which contains admission data for over 900 trauma centers in the United States. Methods: TQIP was queried for adult LEVT patients treated with primary major lower extremity amputation or arterial revascularization from 2017 to 2021. Major amputation was defined by incision above the ankle and below the hip joint. Patients presenting with any traumatic injuries outside the lower extremity were excluded. Demographic, comorbid, and injury-related features were compared between treatment groups. Multivariate logistic regression adjusting for clinical and injury-related covariates was performed to identify factors independently associated with primary amputation. Results: Of 7534 LEVT patients, 743 (9.9%) underwent primary major amputation. Most amputations were above knee (43.4%), followed by below (38.5%) and through knee (16.8%, Figure 1). On univariate analysis, primary amputees were less likely to be Black (23.7 vs 41.9%, p<0.001) and more likely to be privately insured (47.9 vs. 33.9%, p<0.001). Firearms were the most common mechanism of injury in revascularized patients (53.5%) compared to motor vehicle collisions (62.6%) in amputated patients (p <0.001). Time to procedure varied significantly between treatment groups from 15.4 hours in revascularized patients to 139.2 hours in amputated patients. On multivariate logistic regression adjusted for age, race, comorbidities, and injury-related characteristics, blunt mechanism (OR 4.8, p-value < 0.001), tibial arterial injury (OR 2.3, p-value < 0.001), and bony involvement (OR 2.3, p-value < 0.001) were independently associated with primary amputation. Femoral arterial injury (OR 0.4, p-value < 0.001), popliteal injury (OR 0.3, p-value < 0.001), and female sex (OR 0.7, p-value < 0.001) were protective. Conclusion: In the TQIP multicenter registry representing over 900 domestic trauma centers, LEVT patients had a 9.9% primary amputation rate. Primary revascularizations were performed a mean 5 days earlier than amputations, indicating that early vascular care facilitates limb salvage. Blunt tibial arterial injury with bony involvement was independently associated with primary amputation, suggesting that these patients may particularly benefit from expedient vascular evaluation.