OBJECTIVES: Previous research has shown that frailty status does not correlate with 30-day outcomes after repair of a ruptured abdominal aortic aneurysm (rAAA). However, there are no studies to date investigating whether frailty is associated with longer-term mortality and morbidity after rAAA repair. The aim of this study is to evaluate whether frailty can be used as a risk assessment tool for predicting one-year mortality and morbidity in patients undergoing both open and endovascular rAAA repair.
METHODS: We conducted a retrospective analysis of patients undergoing rAAA repair at a single tertiary care center from January 2011 to November 2022. Frailty was assessed for each patient using the modified frailty index (mFI), a validated frailty metric based on the Canadian Study of Health and Aging and was defined as an mFI ≥0.27. The primary outcome was one-year mortality. Logistic regression and receiver operating characteristic (ROC) curves were used to assess mFI-11 with one-year morbidity and mortality. Kaplan-Meier analysis was used to compare rates of survival. Categorical and continuous data were compared using χ2 and Student�s t-tests, respectively. For all tests, a P-value of <0.05 is considered statistically significant.
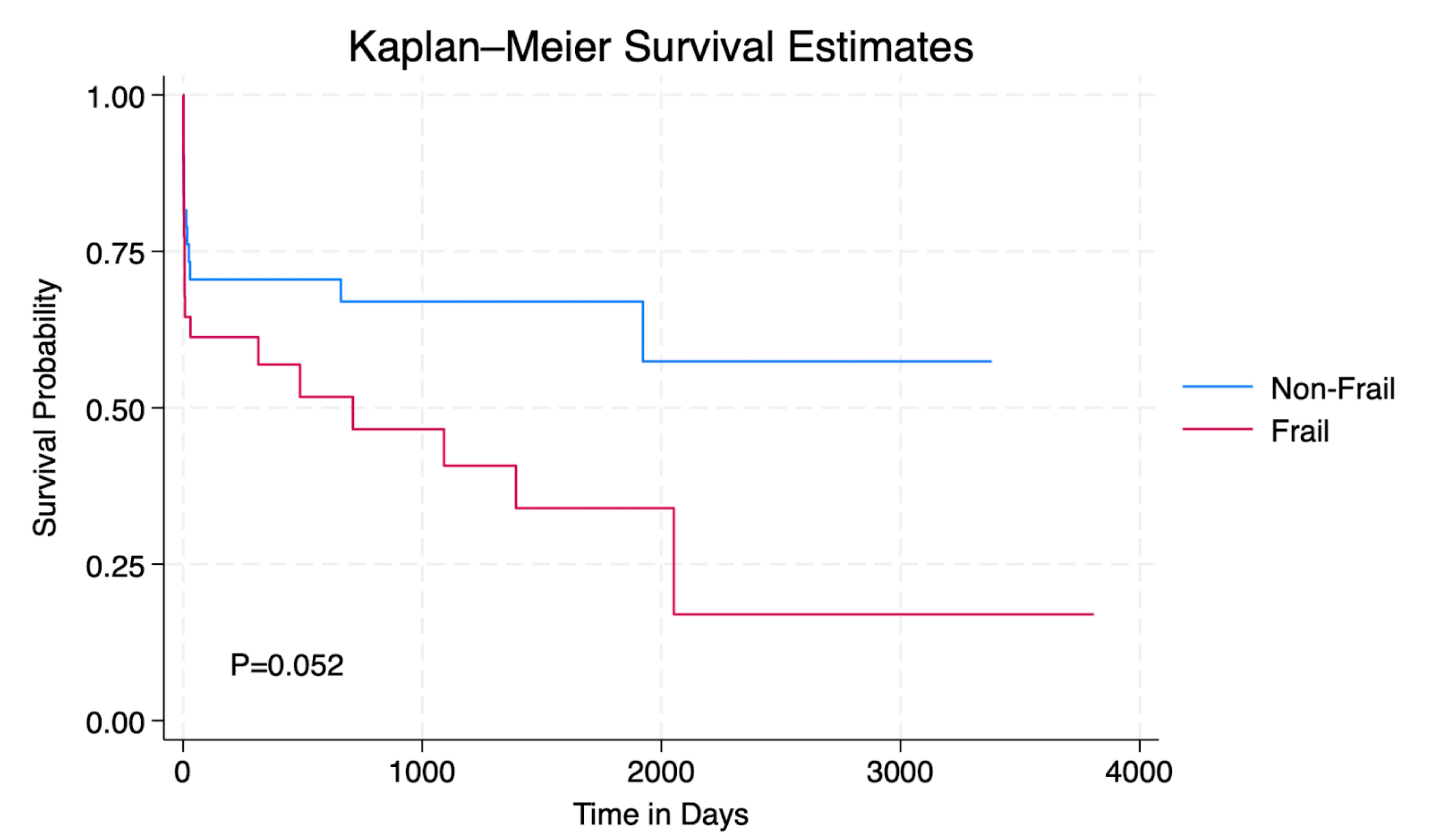
RESULTS:Seventy-eight patients were identified during the study period (35 frail vs. 43 non-frail) with a median follow up of 7 months (5.9 months frail vs. 10 months non-frail) and a one-year mortality rate of 40% overall (49% frail vs. 33% non-frail, P= 0.86). Logistic regression analysis showed no correlation between frailty and reintervention (odds ratio 1.6 [95% confidence interval 0.1-27.6], P=0.75), dialysis dependence (0.8 [0.1-9.2], P=0.83), home oxygen use (1.6 [0.2-13.0], P=0.6), and dependent mobility (0.8 [0.12-4.7], P=0.79). The area under the ROC curve (AUC) for mFI-11 was 0.58 for one-year mortality (P=0.2). Kaplan Meier analysis showed no difference in rates of survival between frail and non-frail patients (P=0.052) (Figure 1).
CONCLUSIONS:Frailty, defined using the modified frailty index, was not predictive of one-year outcomes after open or endovascular rAAA repair. Other metrics are needed to more accurately assess long term risk to enable better patient and family counseling after repair of rAAA.