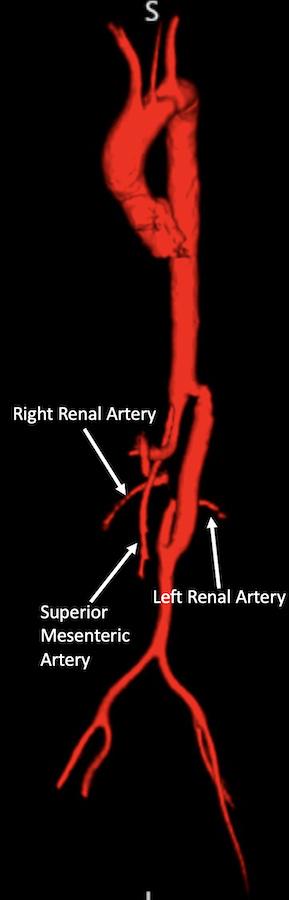
DEMOGRAPHICS: A 46-year-old woman (G1P0) with history of pararenal middle aortic coarctation (MAC) diagnosed at age 2, status post aorto-aortic bypass at age 16, presented to vascular surgery clinic at 8 weeks pregnant with new onset hypertension. Patient�s systolic blood pressures were persistently >150 mmHg despite medical management. Physical exam demonstrated 2+ upper and lower extremity pulses bilaterally. Magnetic resonance arteriogram (MRA) showed a patent bypass with retrograde filling of the left renal artery via the native infrarenal aorta. The right renal artery (RRA) was filling antegrade via the atretic native aorta (Fig 1). Due to the increased risk of maternal/fetal morbidity and mortality, A multidisciplinary discussion determined the patient�s options were early elective termination of pregnancy or hepatorenal bypass for treatment of renovascular hypertension.
HISTORY: Surgery was deferred to the second trimester (16 weeks). A Kocher incision was made followed by a Cattell-Braasch maneuver to expose the right renal hilum. The RRA was exposed at its bifurcation near the hilum and dissected proximally toward its origin at the atretic native aorta. The common hepatic (CHA), gastroduodenal and proper hepatic arteries were dissected and controlled. The left greater saphenous vein (GSV) was harvested. A CHA to RRA bypass was created using reversed GSV in end-to-side fashion. The proximal RRA was ligated at the atretic portion of the coarctation. Intraoperative Doppler confirmed bypass patency with low resistance audible signals.
PLAN: Patients post op recovery was uneventful. She was discharged on day 5 with blood pressure well controlled on Labetalol and remined on this regimen until undergoing cesarean delivery at 32 weeks for pre-eclampsia. Postpartum she was weaned off Labetalol and at 9 and 24 months follow up patient was doing well. Follow up MRA illustrated patent bypass.
DISCUSSION: MAC is a rare diagnosis, but is commonly associated with renal and/or other visceral artery stenoses. Classic presentation is refractory hypertension, lower extremity claudication, and/ or abdominal angina in children or adolescents. This patient underwent CHA to RRA bypass as a last resort treatment for uncontrolled pregnancy induced renovascular hypertension, which if left untreated, would have ultimately led to early pregnancy termination.