DEMOGRAPHICS:This report describes a complex case of a 32 year-old male patient who ultimately underwent infected thoracic endovascular graft and spinal hardware explant with a multidisciplinary team approach.
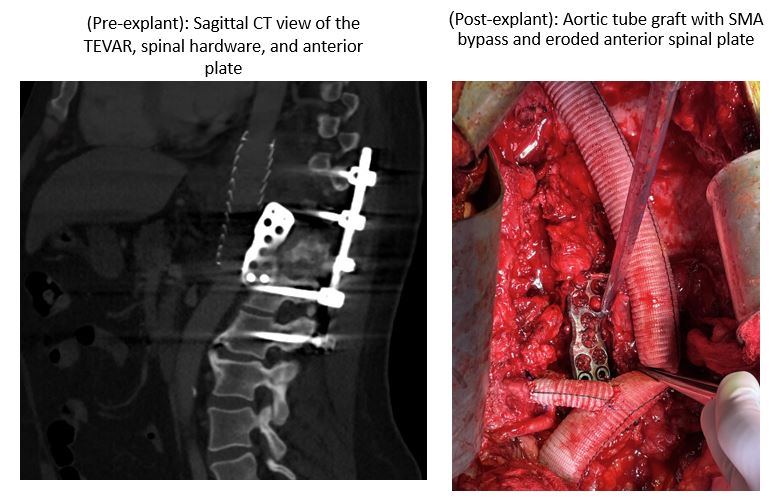
HISTORY:This patient presented to a tertiary referral center with massive hemoptysis with history significant for open anterolateral T10-L2 fusion after suffering a T12 burst fracture a decade ago after rollover motor vehicle accident. He subsequently developed a spinal hardware infection with abscess three years later which was treated nonoperatively. Three years after his spinal hardware infection, he underwent thoracic endovascular repair (Gore� TAG) of a descending aortic pseudoaneurysm at the level of his spinal hardware. His social history was notable for persistent intravenous drug abuse. He had been on long standing suppressive antibiotics for this hardware infection and new endoprosthesis. He presented to our tertiary care facility about six years after the thoracic endovascular aortic repair (TEVAR) with massive hemoptysis. Computed tomography was concerning for an aortobronchial fistula near the level of his endoprosthesis, although there was no evidence of endoleak or pseudoaneurysm. An upper endoscopy was unremarkable but a bronchoscopy showed old blood throughout the lungs. After another episode of massive hemoptysis while hospitalized, he underwent emergent TEVAR. He did well and was discharged two weeks later with plans for definitive explant and reconstruction. PLAN:Two months later he underwent explant of his TEVAR and spinal hardware via a left thoracoabdominal approach. His spinal hardware had eroded through the aortic wall and was excluded by the TEVAR grafts. The vascular and cardiac team reconstructed his descending aorta from the proximal descending aorta to the level of the renals. His celiac artery was occluded from his prior TEVAR and he required a SMA bypass from the aortic tube graft. The neurosurgery team explanted his anterior spinal plate. The thoracic team performed a left lower lobe resection for an aortobronchial fistula and latissimus flap wrap of the laterally tunneled aortic graft. DISCUSSION:This report highlights a complex case of a patient who was temporized with endovascular techniques for a life-threatening complication from a spinal surgery but ultimately underwent successful definitive surgery with a multidisciplinary team.