DemographicsA 73 man with multiple medical comorbidities transferred with Rutherford Category 5 chronic limb threatening ischemia.
HistoryThe patient developed non-healing right foot wounds refractory to local wound care for two months. Non-invasive testing revealed a toe pressure of 26 mmHg. The patient was a high-risk surgical candidate with no adequate great saphenous vein for bypass. Prior attempts at endovascular treatment were unsuccessful due to long segment occlusions so he was transferred for advanced endovascular treatment options.
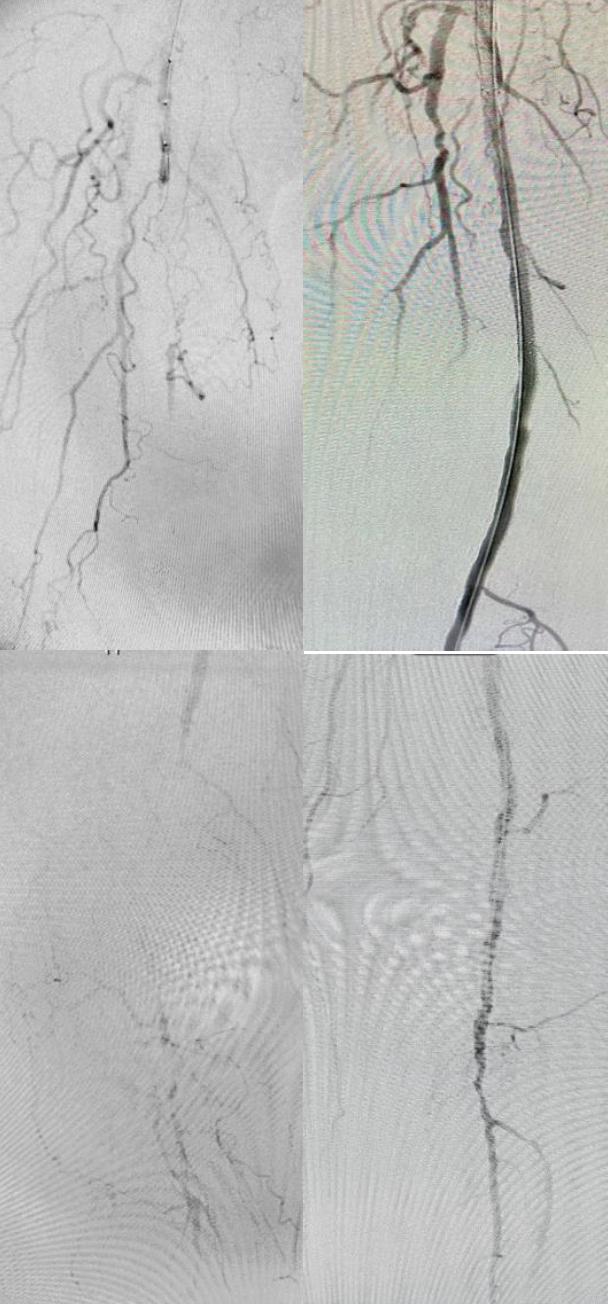
PlanInitial right lower extremity angiogram performed via left groin access demonstrated a 15 cm superficial femoral artery (SFA) occlusion with an island of reconstitution at the adductor hiatus only to reocclude the entire P2 popliteal artery. The tibial run-off consisted of a patent peroneal that collateralized to the distal posterior tibial and anterior tibial artery with mild stenosis throughout to the foot. Initial attempts at crossing the SFA lesion from above were unsuccessful. Using fluoroscopic guidance, the distal right SFA was percutaneously accessed in the patent segment. A 0.018 command wire crossed the occlusion retrograde and was snared from above allowing through and through access. A catheter was brought from above and was confirmed in the true lumen of the distal SFA however crossing the popliteal artery occlusion from above was again unsuccessful. The distal right anterior tibial artery was accessed with ultrasound guidance. A 0.018 command wire crossed the popliteal lesion retrograde and was snared from above for through and through access. Lithotripsy followed by drug coated balloon angioplasty and tacks of the right popliteal artery was performed. The SFA also underwent lithotripsy followed by drug coated stenting. Completion angiography confirmed in-line flow to the foot with no dissections or perforations. 6 month follow-up demonstrated patent repair without significant stenosis, a right toe pressure of 71 mmHg and healed wounds.
Discussion Minimizing long segment subadventitial wire crossing of arterial occlusions allows for a greater breadth of endovascular treatments. Surgeon comfort with retrograde access offers different strategies to crossing challenging lesions. This case highlights the successful use of new endovascular treatments combined with two retrograde accesses for a totally percutaneous operation.