DEMOGRAPHICS: A 41-year-old man with a history of alcohol abuse presented with acute aortic occlusion in the setting of necrotizing pancreatitis.
HISTORY: The patient with a history of alcohol abuse presented to the ER with severe abdominal and back pain. He was frail and unable to walk more than 25 feet due to left hip, thigh, and leg claudication. Initial CT with IV contrast demonstrated necrotizing pancreatitis and chronically occluded left common iliac artery. Within 12 hours of admission, the patient's bilateral lower extremities became mottled and pulseless with sensorimotor deficit. A repeat CTA revealed an acute aortic occlusion from the renal arteries and of the bilateral iliac arterial system.
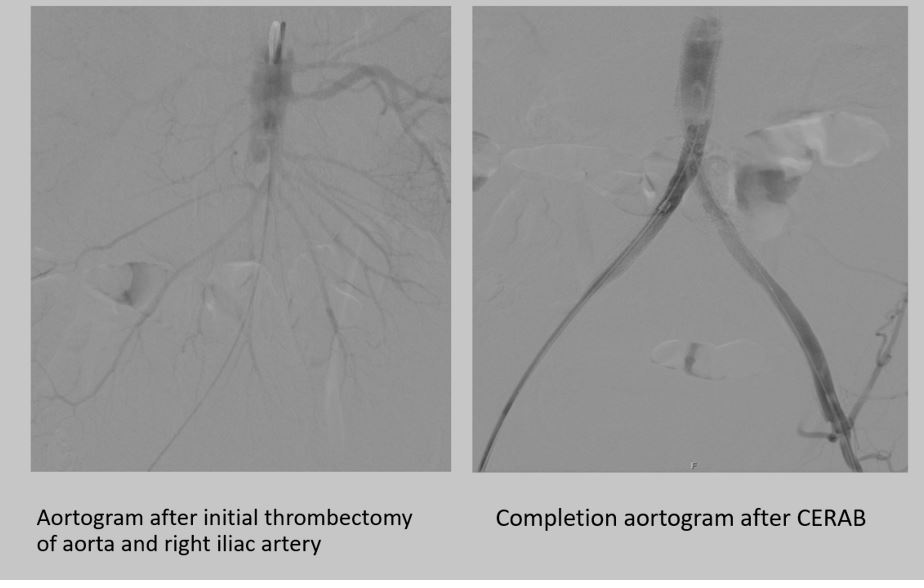
PLAN: The patient underwent emergent bilateral femoral cutdown for aortoiliac thrombectomy. Over the wire Fogarty thrombectomy was performed on the right, however, we were unable to cross the chronically occluded left common iliac lesion. An initial attempt to cross the lesion retrograde with a subintimal technique was performed but we were unable to re-enter the aorta. IVUS demonstrated significant residual thrombus in the aorta, right iliac artery, and a dissected left iliac artery. We then crossed the left iliac artery lesion antegrade using a steerable sheath and externalized the wire. Covered Endovascular Reconstruction of Aortic Bifurcation (CERAB) was performed. An 11 x 79 mm VBX stent graft was placed below the renal arteries and post-dilated with a 16 mm balloon. Bilateral kissing iliac stents were placed at the bifurcation using 8 x 79 mm VBX and post-dilated with 9 mm balloons. The bilateral iliac stents were extended into the external iliac arteries with 8 x 100 mm Viabahn stents. The procedure concluded with 4 compartment bilateral leg fasciotomies. Postoperatively, he required a sigmoidectomy, pancreatic debridement, and temporary hemodialysis but made a complete recovery after 8 weeks. DISCUSSION: Covered Endovascular Reconstruction of Aortic Bifurcation (CERAB) is an excellent option in the management of acute aortic occlusion for inline revascularization. It serves as a great alternative to extra-anatomical bypass and open aortic reconstruction, especially in high-risk patients.