DEMOGRAPHICS45-year-old Caucasian female with hypertension, dyslipidemia, and obesity on semaglutide.
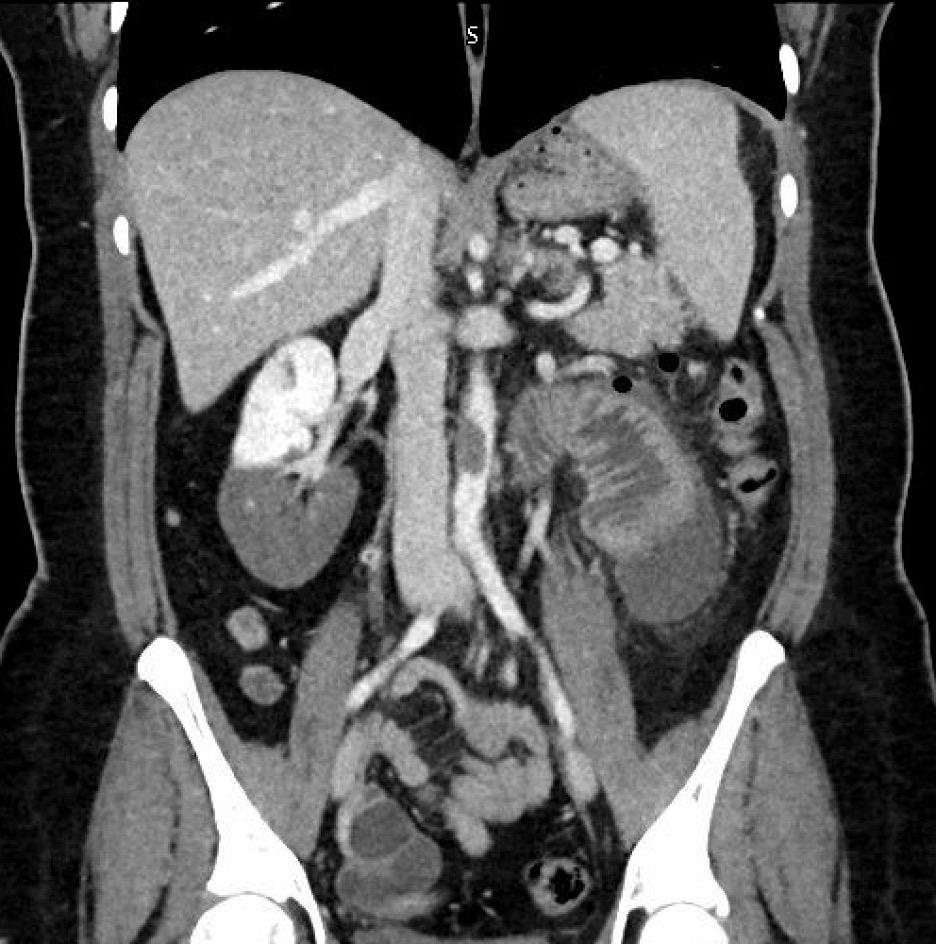
HISTORY: Our patient presented with three months of nausea, vomiting, abdominal pain and anorexia. Cross sectional contrast imaging demonstrated thromboembolic disease in the proximal infrarenal abdominal aorta, superior mesenteric artery (SMA), right renal artery and left common femoral artery.
PLAN: The patient was taken emergently for an endovascular mechanical thrombectomy utilizing the Penumbra thrombectomy system. She underwent mechanical thrombectomy of her infrarenal abdominal aorta utilizing the 16 French Penumbra Flash, and the proximal SMA using the 7 French Penumbra Bolt. Subsequently, we performed a 5mm balloon angioplasty of the proximal SMA.
Next, mechanical thrombectomy of the left common femoral and profunda arteries were performed with a 12 French and 7 French Penumbra catheter, respectively. Repeat angiogram showed good perfusion of the superficial femoral and popliteal arteries; however, there was thromboembolic disease noted in the tibioperoneal trunk and all three distal arteries to the foot. Using the Penumbra 7 French Bolt and the 4 French AngioJet, we performed mechanical thrombectomy as well as administered tPA into all 3 tibial vessels removing significant thrombus, with return of three vessel runoff.
The following day, the patient had absent doppler signals in the right lower extremity. A right ankle level AT and PT artery cutdown with Fogarty embolectomies were performed.
A hypercoagulable workup was completed, and the patient is positive for a Jak2 V617F mutation.
DISCUSSION We believe that this patient had a primary in situ aortic thrombosis that embolized distally, with a concomitant SMA thrombus.
The JAK2 V617F mutation is an acquired, somatic mutation. The presence of JAK2 V617F mutation has been shown to increase the relative risk for arterial thrombosis 5-fold and patients
often have thrombotic events in the absence of other clinical or laboratory evidence. While this patient was found to have a JAK2 V617F mutation, the presence of concomitant inherited thrombophilia cannot be ruled out without confirmatory bone marrow biopsy.
Figure 1. Cross Sectional Imaging demonstrating Infrarenal Aortic Thrombus, Left common femoral Thrombus, and Right Renal Infarct