|
Back to Annual Symposium Program
Bowing As An Adjunct For Endovascular Aneurysm Repair
Chen Rubinstein, MD, Eric D. Endean, MD, David J. Minion, MD, Gabriel J. Bietz, MD, Ehab S. Sorial, MD, Shane D. O'Keeffe, MD, Eleftherios S. Xenos, MD, PhD.
University of Kentucky, Lexington, KY, USA.
Objectives:
Commercially available devices for endoluminal abdominal aortic aneurysm (AAA) repair are limited to proximal neck angle ≤ 60°. We herein report a case of a patient with 90° angulation at the proximal neck and describe a method in order to overcome this limitation.
Methods:
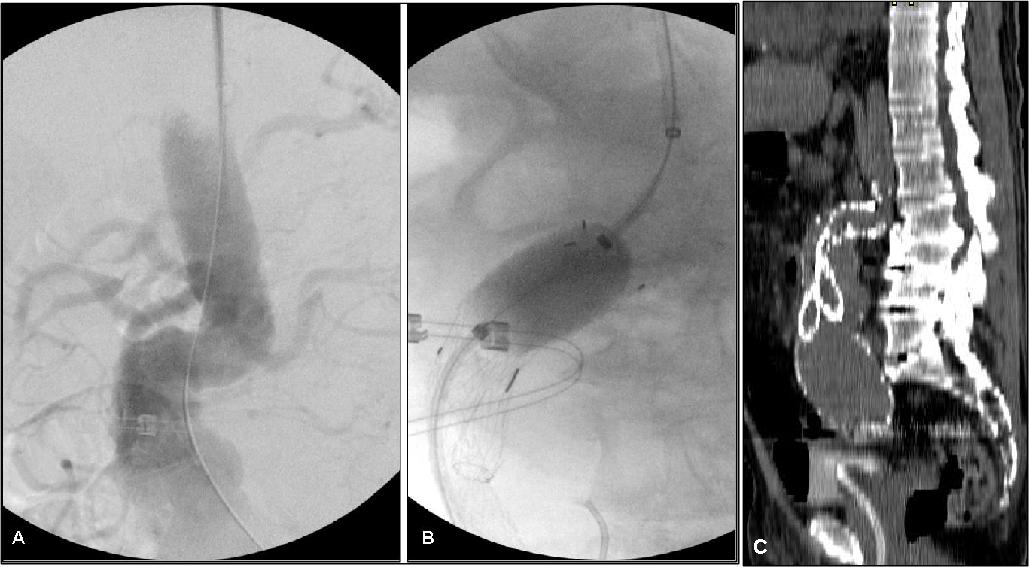
Case report. A 82 year old male with multiple medical comorbidities presented with a 7.1cm infrarenal AAA and a 7.2cm, and 3.4cm right and left common iliac aneurysms respectively. As his proximal neck angle was 90°, we elected to occlude his hypogastric arteries bilaterally and stage the aneurysm repair. Neck length was 3.6cm. Two weeks after successful embolization of the left hypogastric, he underwent endoluminal aneurysm repair. The femoral arteries were accessed bilaterally as well as the left axillary artery. A Glide-wire® was inserted via the axillary approach and snared from the groin. A long catheter was used to exchange this wire to a stiff wire (Amplatz Stiff Wire®). As the right hypogastric was big and tortuous we elected to fill it with Amplatzer Plugs® and Onyx® in order to prevent type II endoleak from the hypogastric artery. Further steps in the procedure were performed in the standard fashion, however prior to positioning and deployment of the graft, pushing motion was applied to the stiff wire from both directions in order for it to bow and better conform to the curves of the native aorta. This pushing motion from above and below was also applied in order to facilitate advancement of the stent-graft and placing it perpendicular to the long axis of the aorta, conforming to the angulation of the neck (image A - neutral position, B - with bowing).
Results:
Using this maneuver, and the Gore Excluder® stent graft system, we were able to successfully complete the endovascular repair. Standard bilateral groin approach would not enable us to place the stents in the proper plane, in order to achieve adequate seal (post-op CT, image C).
Conclusions:
Wire bowing assists in achieving good apposition and proximal seal in the presence of sharp angulation. 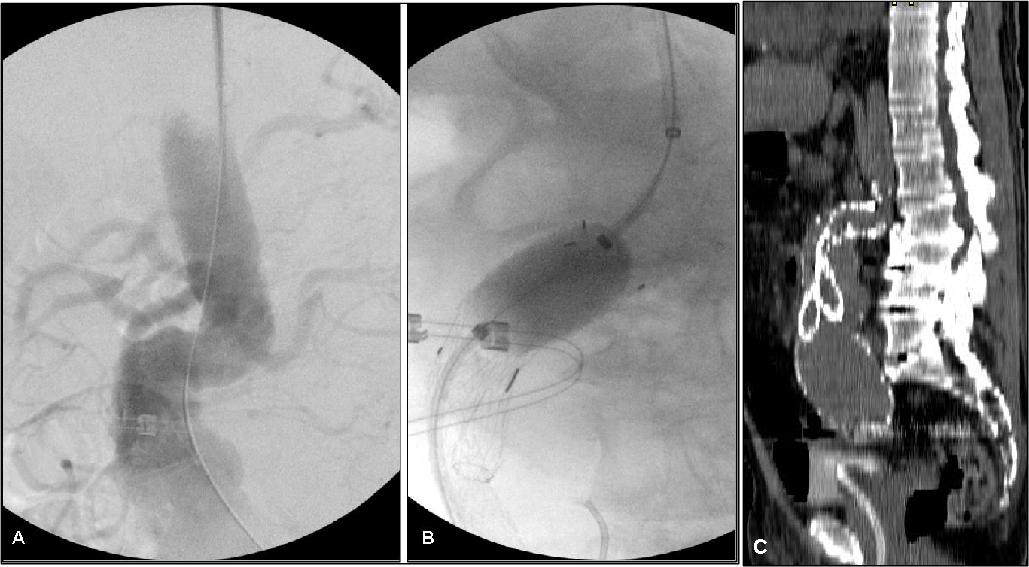
Back to Annual Symposium Program

|