Back to ePosters
Percutaneous thrombolysis of acute-on-chronic IVC thrombosis after previous insertion of an Adams-DeWeese Clip
Mark E. O'Donnell, MMedSc MD FRCS, Sailendra G. Naidu, MD, Kathryn E. Coan, MD, Grant T. Fankhauser, MD, Richard J. Fowl, MD, William M. Stone, MD, Fadi E. Shamoun, MD, Samuel R. Money, MD.
Mayo Clinic, Phoenix, AZ, USA.
OBJECTIVES: Complete IVC interruption for pulmonary emboli (PE) prophylaxis was replaced by partial interruption procedures to minimize acute cardiovascular collapse and chronic venous insufficiency complications whereby the Adams-DeWeese clip was developed.
METHODS: We describe the successful percutaneous treatment of acute-on-chronic IVC thrombosis thirty-one years following previous placement of Adams-DeWeese clip.
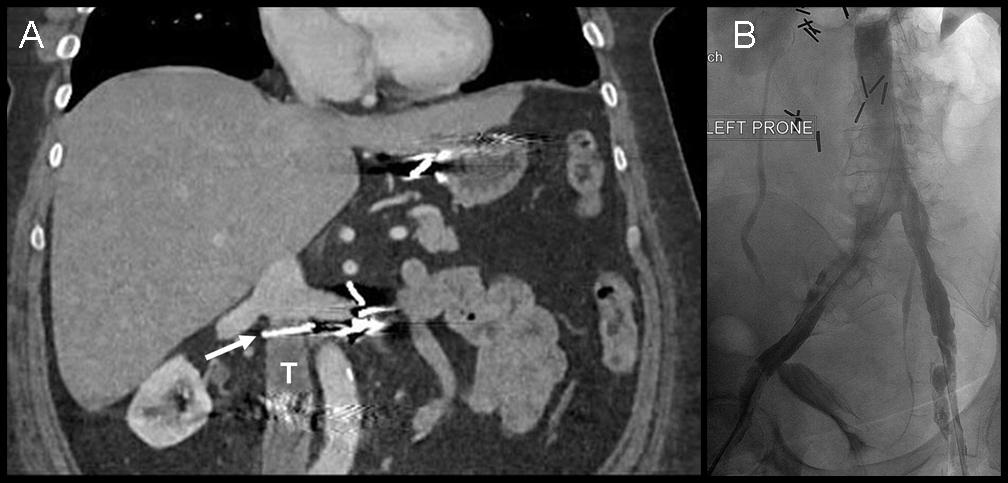
RESULTS: A 60-year old female nurse presented with a ten-day history of increasing back pain,bilateral lower extremity edema and a significant weight gain with progressive dyspnea.She had known protein C deficiency and an Adams-DeWeese Clip had been previously placed following multiple PE after complications of gastric bypass surgery thirty-one years previously. She was initially on Coumadin for two-years before switching to aspirin 325mg daily.She was a non-smoker.She was hemodynamcially stable with normal breath sounds and bilateral lower limb edema. Venous duplex revealed bilateral lower extremity occlusive thrombosis extending to the common femoral vein.CT venography confirmed thrombus extending superiorly to the infrarenal IVC adjacent to the previously inserted Adams-DeWeese clip(Figure 1). The patient was commenced on a therapeutic heparin infusion. Venography performed for severe symptomatology confirmed significant IVC clot burden which was treated with pulse spray tissue plasminogen activator (tPA) followed by percutanous mechanical thrombectomy (Angiojet®, Possis Medical). Two high-grade right superficial femoral vein stenoses were treated with balloon angioplasty. Two weeks later repeat imaging confirmed IVC thrombus recurrence which was treated with a twenty-four hour tPA infusion following placement of two 50cm infusion catheters (AngioDynamics Uni-fuse™) below the Adams-DeWeese clip. Residual clot burden the next day required mechanical thrombectomy. Partially improved flow necessitated a further tPA and heparin infusion. Continued IVC poor flow on day-three required passage of bilateral stiff angled Glidewires proximally through two fenestrations in the Adams-DeWeese clip. Repeat mechanical thrombectomies followed by sequential balloon venoplasty through the Adams-DeWeese clip fenestrations finally improved flow(Figure 1). The patient remains mobile two years later and continues with compression hosiery and lifelong anticoagulation.
CONCLUSIONS: Although the current prevalence of patients with in-situ IVC interruption devices remains unknown, clinical symptomatology may only present following additional precipitating events often requiring multiple procedures using a myriad of modalities in conjunction with long-term anticoagulation treatment.
Back to ePosters

|
