
Advanced endovascular snare technique to cross high-grade common iliac artery stenosis or occlusion
Kathleen M. Lamb, MD, Jon Quatromoni, MD, Philip Batista, MD, Paul Foley, MD.
Hospital of the University of Pennsylvania, Philadelphia, PA, USA.
OBJECTIVE: Severe CIA stenosis or occlusion leads to limb ischemia resulting in debilitating claudication, rest pain, or tissue loss. Recanilization can be achieved with endovascular techniques. In cases of severe iliac stenosis or occlusion, crossing these lesions may prove technically challenging. Herein, we present the application of an AEST to cross long-segment CIA occlusions utilizing bilateral femoral access.
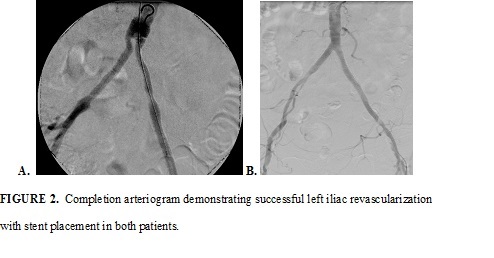
METHODS: Two patients presented with TASC-D left CIA occlusions manifesting with severe buttock and leg claudication (Figure 1). In both cases, initial attempts at recanalization involved retrograde puncture of the common femoral artery (CFA) ipsilateral to iliac occlusion. Despite use of multiple catheters and wires, these lesions were unable to be crossed from a retrograde approach. Subsequently retrograde puncture of contralateral CFA was performed, followed by successful crossing of the iliac occlusions using an up-and-over approach with a stiff glide wire and catheter. With the lesions crossed, a snare device was inserted from the ipsilateral groin and was used to snare the crossing wire from the contralateral groin. The wire was then pulled out through the sheath in the ipsilateral groin thus establishing a platform for ipsilateral retrograde access. A stiff wire was placed across the lesions to allow for deployment of Atrium iCAST stents, thus restoring flow.
RESULTS: A successful angiographic result was obtained in both patients (Figure 2). They were discharged home on aspirin and clopidogrel on post-operative day 2 and 5 respectively with resolution of their claudication. Each patient was then seen in clinic at 1 month with ABI/PVRs to confirm continued patency and normal triphasic waveforms below the stent.
CONCLUSIONS: Severe CIA stenosis or occlusion remains challenging to cross with routine endovascular techniques. AEST utilizing bilateral femoral artery access may assist in establishing retrograde access across the lesion to permit endovascular intervention in cases where it otherwise would not have been feasible .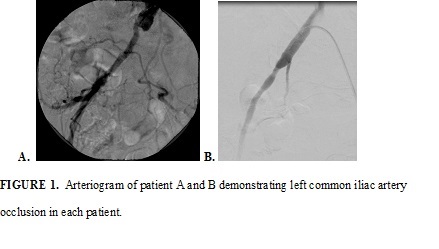
Back to 2017 Karmody Posters



