
Preoperative anemia increases the risk of mortality in symptomatic patients undergoing carotid endarterectomy.
Alexander B. Pothof, MSc, MD1, Thomas C.F. Bodewes, MD1, Jeremy D. Darling, BA1, Sarah Deery, MD1, Katie E. Shean, MD1, Peter A. Soden, MD1, Gert J. de Borst, MD2, Marc L. Schermerhorn, MD1.
1BIDMC, Boston, MA, USA, 2UMCU, Utrecht, Netherlands.
Objectives: The impact of anemia and blood transfusion on carotid endarterectomy (CEA) is unknown.
Methods: All CEAs from 2011-2014 in the Targeted Vascular NSQIP were stratified by symptom status and preoperative anemia (hematocrit <35). Multivariable analysis accounted for differences in demographics and comorbidities. We included an interaction term to assess effect modification between anemia and postoperative transfusion.
Results: Of 12407 CEA patients, 5173(42%) were symptomatic, of whom 900(17%) had anemia; of these 10% were transfused vs. 0.5% of non-anemic patients. Of 6089 asymptomatic patients, 1145(16%) had anemia, of whom 7.7% were transfused vs. 0.8% of non-anemic patients. Symptomatic patients with anemia, compared to those without anemia had higher stroke/death (5.8% vs. 3.4%, p=.01) and mortality (2.7% vs. 0.7%, p<.001), stroke was similar. In asymptomatic patients there were no differences in stroke/death, mortality or stroke between anemic and non-anemic patients. After adjustment, symptomatic patients with anemia had a higher risk of death (OR:2.5, 95%CI:1.4-4.6, p=.002), but not stroke/death or stroke (Table). In asymptomatic patients, anemia was not associated with stroke/death, mortality, or stroke. In our interaction model, compared to patients without anemia or postoperative transfusion, symptomatic patients with both anemia and postoperative transfusion had an increased risk of mortality (OR:5.5, 95%CI:2.0-15, p=.001), but not of stroke/death (OR:1.7, 95%CI:0.7-4.0, p=.2) or stroke (OR:0.7, 95%CI:0.2-2.7, p=.6). For asymptomatic patients, anemia with postoperative transfusion was associated with stroke/death ((OR:4.3, 95%CI:1.8-10, p=.001), mortality (OR:4.8, 95%CI:1.4-17, p=.01) and stroke (OR:3.5, 95%CI:1.1-12, p=.04). In those without anemia, postoperative transfusion was associated with increased risk of stroke/death, and stroke for both symptomatic (OR:6.8, 95%CI:2.5-19, p=<.001; OR:6.4, 95%CI:2.1-19, p=.001) and asymptomatic patients (OR:8.1, 95%CI:3.4-20, p=<.001; OR:11, 95%CI:4.1-28, p<.001).
Conclusions: Preoperative anemia increases the risk of mortality in symptomatic patients, and its effect is amplified by postoperative transfusion. For asymptomatic patients, only anemia with postoperative transfusion is associated with an increased risk of stroke/death, mortality and stroke. Postoperative transfusion without anemia is associated with an increased risk of stroke/death and mortality. Further analysis to determine optimal management of anemia in pre-operative and post-operative patients with carotid stenosis is needed. 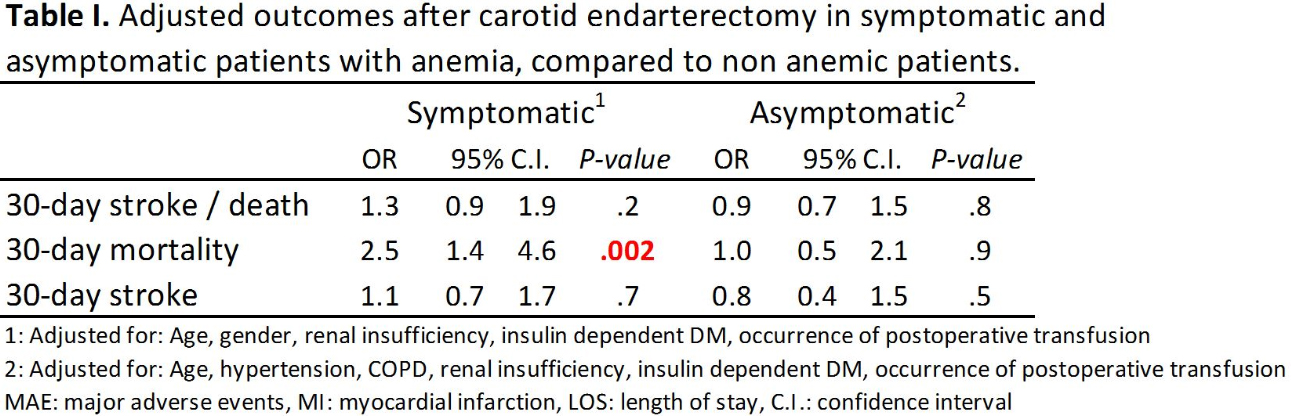
Back to 2017 Program



